

Ventilator-Associated Pneumonia due to Drug-Resistant Acinetobacter baumannii: Risk Factors and Mortality Relation with Resistance Profiles, and Independent Predictors of In-Hospital Mortality
- PMID: 30781896
- PMCID: PMC6410055
- DOI: 10.3390/medicina55020049
Ventilator-Associated Pneumonia due to Drug-Resistant Acinetobacter baumannii: Risk Factors and Mortality Relation with Resistance Profiles, and Independent Predictors of In-Hospital Mortality
Abstract
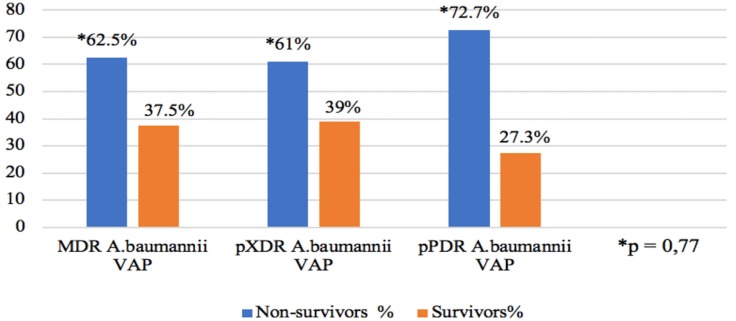
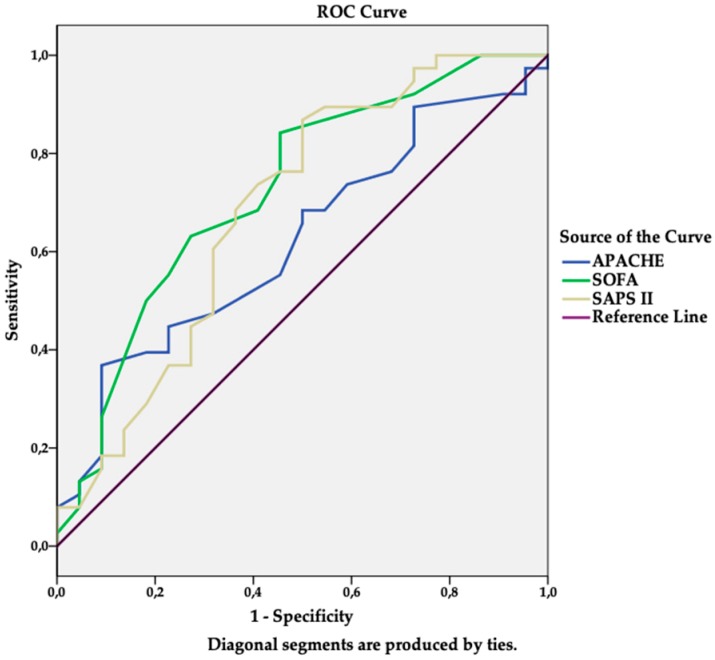
Background and objectives: High mortality and healthcare costs area associated with ventilator-associated pneumonia (VAP) due to Acinetobacter baumannii (A. baumannii). The data concerning the link between multidrug-resistance of A. baumannii strains and outcomes remains controversial. Therefore, we aimed to identify the relation of risk factors for ventilator-associated pneumonia (VAP) and mortality with the drug resistance profiles of Acinetobacter baumannii (A. baumannii) and independent predictors of in-hospital mortality. Methods: A retrospective ongoing cohort study of 60 patients that were treated for VAP due to drug-resistant A. baumannii in medical-surgical intensive care units (ICU) over a two-year period was conducted. Results: The proportions of multidrug-resistant (MDR), extensively drug-resistant (XDR), and potentially pandrug-resistant (pPDR) A. baumannii were 13.3%, 68.3%, and 18.3%, respectively. The SAPS II scores on ICU admission were 42.6, 48.7, and 49 (p = 0.048); hospital length of stay (LOS) prior to ICU was 0, one, and two days (p = 0.036), prior to mechanical ventilation (MV)-0, 0, and three days (p = 0.013), and carbapenem use prior to VAP-50%, 29.3%, and 18.2% (p = 0.036), respectively. The overall in-hospital mortality rate was 63.3%. In MDR, XDR, and pPDR A. baumannii VAP groups, it was 62.5%, 61.3%, and 72.7% (p = 0.772), respectively. Binary logistic regression analysis showed that female gender (95% OR 5.26; CI: 1.21⁻22.83), SOFA score on ICU admission (95% OR 1.28; CI: 1.06⁻1.53), and RBC transfusion (95% OR 5.98; CI: 1.41⁻25.27) were all independent predictors of in-hospital mortality. Conclusions: The VAP risk factors: higher SAPS II score, increased hospital LOS prior to ICU, and MV were related to the higher resistance profile of A. baumannii. Carbapenem use was found to be associated with the risk of MDR A. baumannii VAP. Mortality due to drug-resistant A. baumannii VAP was high, but it was not associated with the A. baumannii resistance profile. Female gender, SOFA score, and RBC transfusion were found to be independent predictors of in-hospital mortality.
Keywords: A. baumannii; drug resistance; mortality; predictors; ventilator-associated pneumonia (VAP).
Conflict of interest statement
Rello served in the speaker’s bureau or consultant for Pfizer, Novartis, ROCHE. The remaining authors declare that they have no competing interests.
Figures
References
-
- Li Y.J., Pan C.Z., Fang C.Q., Zhao Z.X., Chen H.L., Guo P.H., Zhao Z.W. Pneumonia caused by extensive drug-resistant Acinetobacter baumannii among hospitalized patients: Genetic relationships, risk factors and mortality. BMC Infect. Dis. 2017;17:371. doi: 10.1186/s12879-017-2471-0. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
