

Impact of renal dysfunction on the management and outcome of acute heart failure: results from the French prospective, multicentre, DeFSSICA survey
- PMID: 30782685
- PMCID: PMC6340446
- DOI: 10.1136/bmjopen-2018-022776
Impact of renal dysfunction on the management and outcome of acute heart failure: results from the French prospective, multicentre, DeFSSICA survey
Abstract
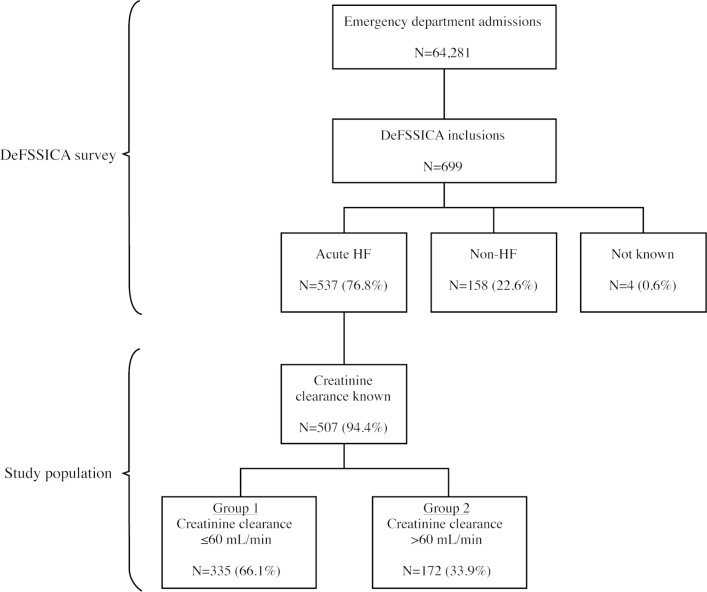
Objectives: Cardiorenal syndrome (CRS) is the combination of acute heart failure syndrome (AHF) and renal dysfunction (creatinine clearance (CrCl) ≤60 mL/min). Real-life data were used to compare the management and outcome of AHF with and without renal dysfunction.
Design: Prospective, multicentre.
Setting: Twenty-six academic, community and regional hospitals in France.
Participants: 507 patients with AHF were assessed in two groups according to renal function: group 1 (patients with CRS (CrCl ≤60 mL/min): n=335) and group 2 (patients with AHF with normal renal function (CrCl >60 mL/min): n=172).
Results: Differences were observed (group 1 vs group 2) at admission for the incidence of chronic heart failure (56.42% vs 47.67%), use of furosemide (60.9% vs 52.91%), insulin (15.52% vs 9.3%) and amiodarone (14.33% vs 4.65%); additionally, more patients in group 1 carried a defibrillator (4.78% vs 0%), had ≥2 hospitalisations in the last year (15.52% vs 5.81%) and were under the care of a cardiologist (72.24% vs 61.63%). Clinical signs were broadly similar in each group. Brain-type natriuretic peptide (BNP) and BNP prohormone were higher in group 1 than group 2 (1157.5 vs 534 ng/L and 5120 vs 2513 ng/mL), and more patients in group 1 were positive for troponin (58.2% vs 44.19%), had cardiomegaly (51.04% vs 37.21%) and interstitial opacities (60.3% vs 47.67%). The only difference in emergency treatment was the use of nitrates, (higher in group 1 (21.9% vs 12.21%)). In-hospital mortality and the percentage of patients still hospitalised after 30 days were similar between groups, but the median stay was longer in group 1 (8 days vs 6 days).
Conclusions: Renal impairment in AHF should not limit the use of loop diuretics and/or vasodilators, but early assessment of pulmonary congestion and close monitoring of the efficacy of conventional therapies is encouraged to allow rapid and appropriate implementation of alternative therapies if necessary.
Keywords: acute heart Failure; ahf; cardio-renal syndrome; crs; real-life; renal dysfunction.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: CEK has received grants from Novartis (other than this work), Daiichy Sankyo and Boehringer Ingleheim. NP report has acted as a paid consultant for Vygon SA. SC reports personal fees from Novartis (other than this work). LF is an employee of RESCUe Network.
Figures
References
-
- Ferreira JP, Girerd N, Pellicori P, et al. . Renal function estimation and Cockroft-Gault formulas for predicting cardiovascular mortality in population-based, cardiovascular risk, heart failure and post-myocardial infarction cohorts: The Heart ‘OMics’ in AGEing (HOMAGE) and the high-risk myocardial infarction database initiatives. BMC Med 2016;14:181 10.1186/s12916-016-0731-2 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous