

Incidence of Acute Kidney Injury in Critically Ill Patients Receiving Vancomycin with Concomitant Piperacillin-Tazobactam, Cefepime, or Meropenem
- PMID: 30782987
- PMCID: PMC6496064
- DOI: 10.1128/AAC.02658-18
Incidence of Acute Kidney Injury in Critically Ill Patients Receiving Vancomycin with Concomitant Piperacillin-Tazobactam, Cefepime, or Meropenem
Abstract
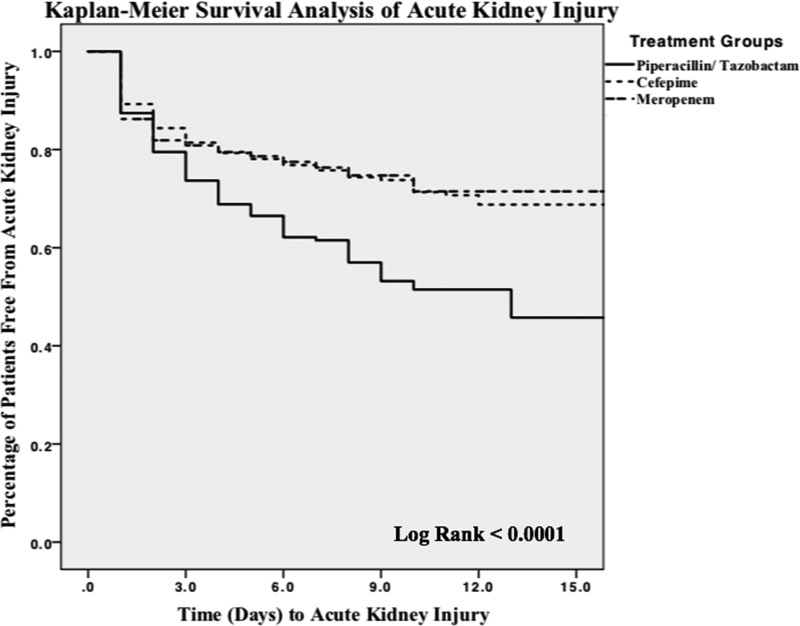
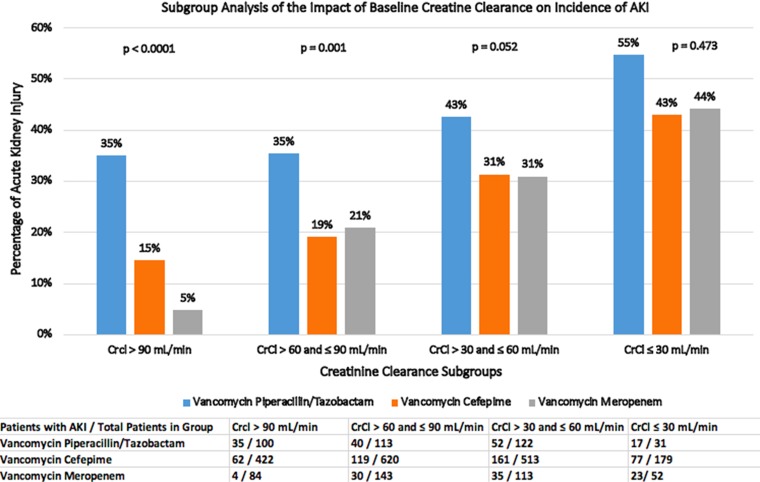
Critically ill patients are frequently treated with empirical antibiotic therapy, including vancomycin and β-lactams. Recent evidence suggests an increased risk of acute kidney injury (AKI) in patients who received a combination of vancomycin and piperacillin-tazobactam (VPT) compared with patients who received vancomycin alone or vancomycin in combination with cefepime (VC) or meropenem (VM), but most studies were conducted predominately in the non-critically ill population. A retrospective cohort study that included 2,492 patients was conducted in the intensive care units of a large university hospital with the primary outcome being the development of any AKI. The rates of any AKI, as defined by the Kidney Disease: Improving Global Outcomes (KDIGO) guidelines, were 39.3% for VPT patients, 24.2% for VC patients, and 23.5% for VM patients (P < 0.0001 for both comparisons). Similarly, the incidences of stage 2 and stage 3 AKI were also significantly higher for VPT patients than for the patients in the other groups. The rates of stage 2 and stage 3 AKI, respectively, were 15% and 6.6% for VPT patients, 5.8% and 1.8% for VC patients, and 6.6% and 1.3% for VM patients (P < 0.0001 for both comparisons). In multivariate analysis, the use of vancomycin in combination with piperacillin-tazobactam was found to be an independent predictor of AKI (odds ratio [OR], 2.161; 95% confidence interval [CI], 1.620 to 2.883). In conclusion, critically ill patients receiving the combination of VPT had the highest incidence of AKI compared to critically ill patients receiving either VC or VM.
Keywords: acute kidney injury; cefepime; meropenem; piperacillin-tazobactam; vancomycin.
Copyright © 2019 American Society for Microbiology.
Figures
References
-
- Rhodes A, Evans LE, Alhazzani W, Levy MM, Antonelli M, Ferrer R, Kumar A, Sevransky JE, Sprung CL, Nunnally ME, Rochwerg B, Rubenfeld GD, Angus DC, Annane D, Beale RJ, Bellinghan GJ, Bernard GR, Chiche J-D, Coopersmith C, De Backer DP, French CJ, Fujishima S, Gerlach H, Hidalgo JL, Hollenberg SM, Jones AE, Karnad DR, Kleinpell RM, Koh Y, Lisboa TC, Machado FR, Marini JJ, Marshall JC, Mazuski JE, McIntyre LA, McLean AS, Mehta S, Moreno RP, Myburgh J, Navalesi P, Nishida O, Osborn TM, Perner A, Plunkett CM, Ranieri M, Schorr CA, Seckel MA, Seymour CW, Shieh L, Shukri KA, Simpson S, Singer M, Thompson S, Townsend B, Van der Poll T, Vincent J-L, Wiersinga W, Zimmerman J, Dellinger R. 2017. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock: 2016. Crit Care Med 45:486–552. doi: 10.1097/CCM.0000000000002255. - DOI - PubMed
-
- Kalil AC, Metersky ML, Klompas M, Muscedere J, Sweeney DA, Palmer LB, Napolitano LM, O'Grady NP, Bartlett JG, Carratalà J, El Solh AA, Ewig S, Fey PD, File TM Jr, Restrepo MI, Roberts JA, Waterer GW, Cruse P, Knight SL, Brozek JL. 2016. Management of adults with hospital acquired and ventilator associated pneumonia: 2016 clinical practice guidelines by the Infectious Disease Society of America and the American Thoracic Society. Clin Infect Dis 63:e61–e111. doi: 10.1093/cid/ciw353. - DOI - PMC - PubMed
-
- Hoste EA, Bagshaw SM, Bellomo R, Cely CM, Colman R, Cruz DN, Edipidis K, Forni LG, Gomersall CD, Govil D, Honoré PM, Joannes-Boyau O, Joannidis M, Korhonen AM, Lavrentieva A, Mehta RL, Palevsky P, Roessler E, Ronco C, Uchino S, Vazquez JA, Vidal Andrade E, Webb S, Kellum JA. 2015. Epidemiology of acute kidney injury in critically ill patients: The multinational AKI-EPI study. Intensive Care Med 41:1411–1423. doi: 10.1007/s00134-015-3934-7. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
