

CD8+ T cells from patients with narcolepsy and healthy controls recognize hypocretin neuron-specific antigens
- PMID: 30783092
- PMCID: PMC6381094
- DOI: 10.1038/s41467-019-08774-1
CD8+ T cells from patients with narcolepsy and healthy controls recognize hypocretin neuron-specific antigens
Abstract
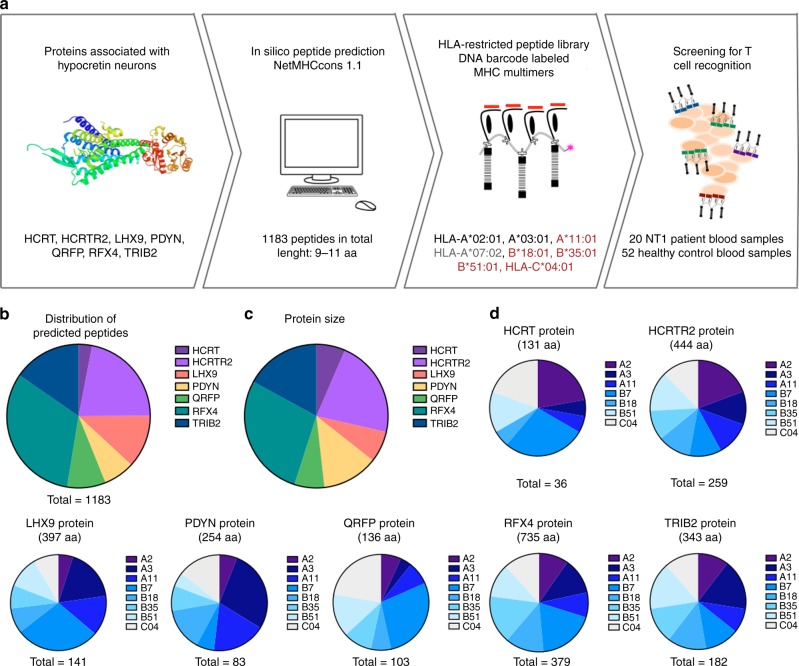
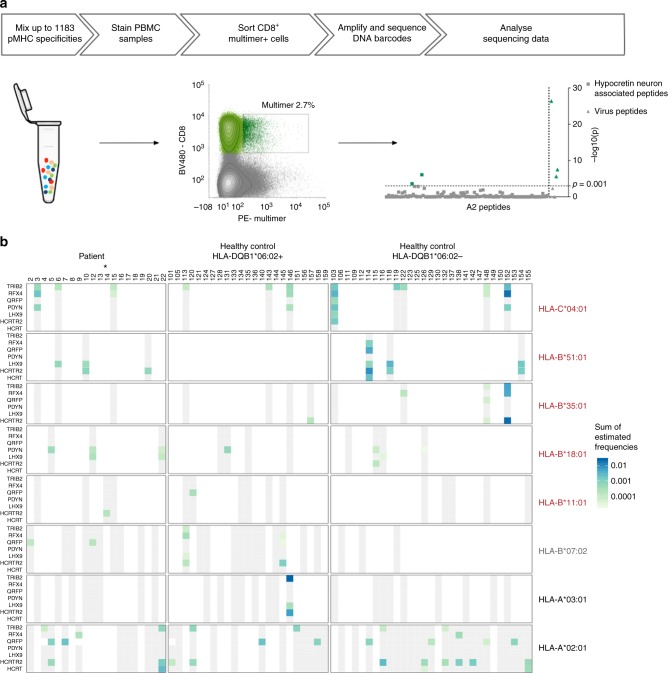
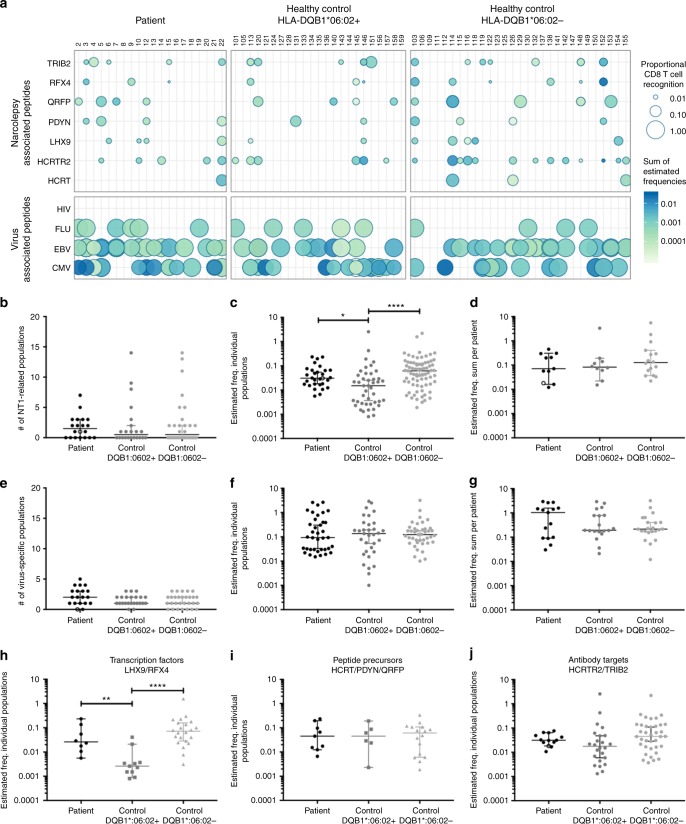
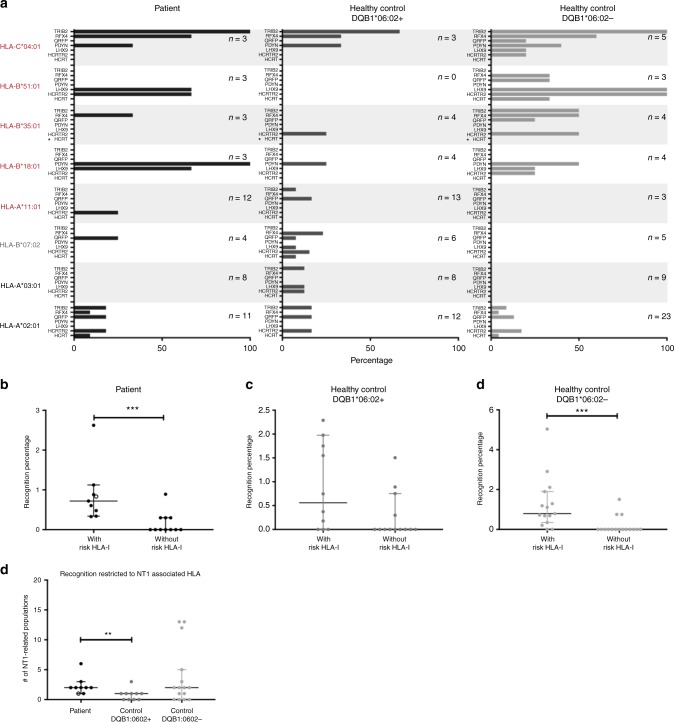
Narcolepsy Type 1 (NT1) is a neurological sleep disorder, characterized by the loss of hypocretin/orexin signaling in the brain. Genetic, epidemiological and experimental data support the hypothesis that NT1 is a T-cell-mediated autoimmune disease targeting the hypocretin producing neurons. While autoreactive CD4+ T cells have been detected in patients, CD8+ T cells have only been examined to a minor extent. Here we detect CD8+ T cells specific toward narcolepsy-relevant peptides presented primarily by NT1-associated HLA types in the blood of 20 patients with NT1 as well as in 52 healthy controls, using peptide-MHC-I multimers labeled with DNA barcodes. In healthy controls carrying the disease-predisposing HLA-DQB1*06:02 allele, the frequency of autoreactive CD8+ T cells was lower as compared with both NT1 patients and HLA-DQB1*06:02-negative healthy individuals. These findings suggest that a certain level of CD8+ T-cell reactivity combined with HLA-DQB1*06:02 expression is important for NT1 development.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
Research Materials
