

Preoperative rectosigmoid endoscopic ultrasonography predicts the need for bowel resection in endometriosis
- PMID: 30783373
- PMCID: PMC6378538
- DOI: 10.3748/wjg.v25.i6.696
Preoperative rectosigmoid endoscopic ultrasonography predicts the need for bowel resection in endometriosis
Abstract
Background: Rectosigmoid endometriosis is an underdiagnosed disease responsible for abdominal pain, transit disorders and rectal bleeding. Two surgical approaches, rectosigmoid bowel resection (segmental or patch) or intramuscular layer dissection (shaving), are available.
Aim: To assess whether the lesion features observed via preoperative rectosigmoid endoscopic ultrasonography (RS-EUS) might predict the need for bowel resection.
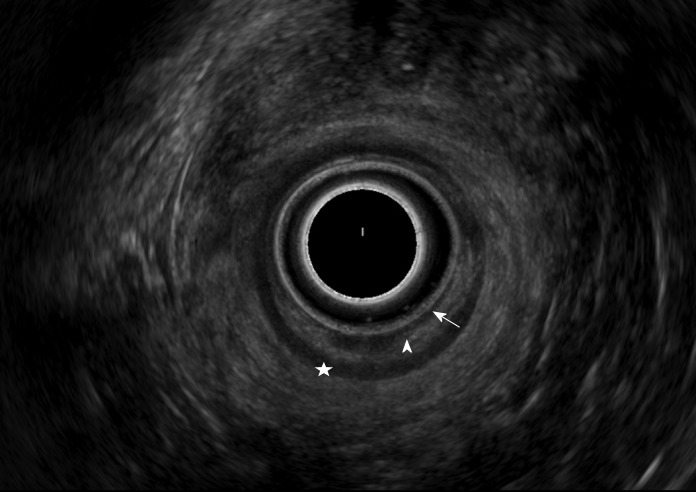
Methods: This multicentric retrospective study was conducted on patients with rectosigmoid endometriosis who underwent a curative surgical procedure, evaluated by RS-EUS performed by two trained operators, between January 2012 and March 2018. A univariate statistical analysis was performed on nodules' RS-EUS features (thickness, width, infiltration of the submucosae, presence of a bump into the digestive lumen and presence of multiple rectosigmoid localizations). A multivariate logistic regression was then performed on the significant results.
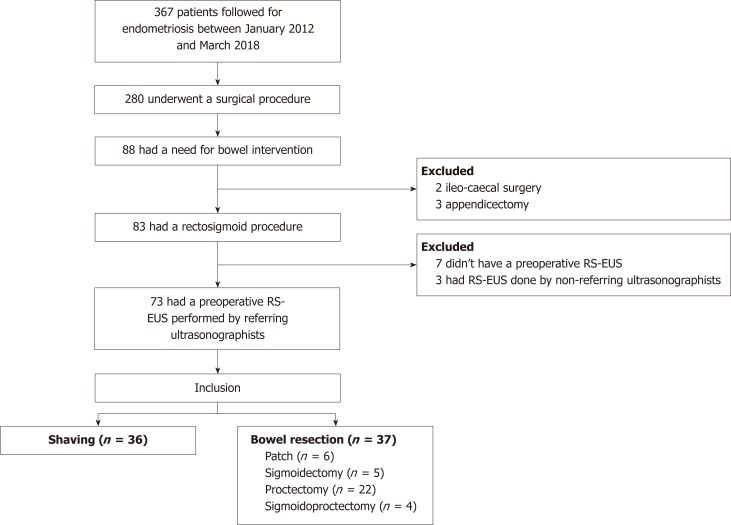
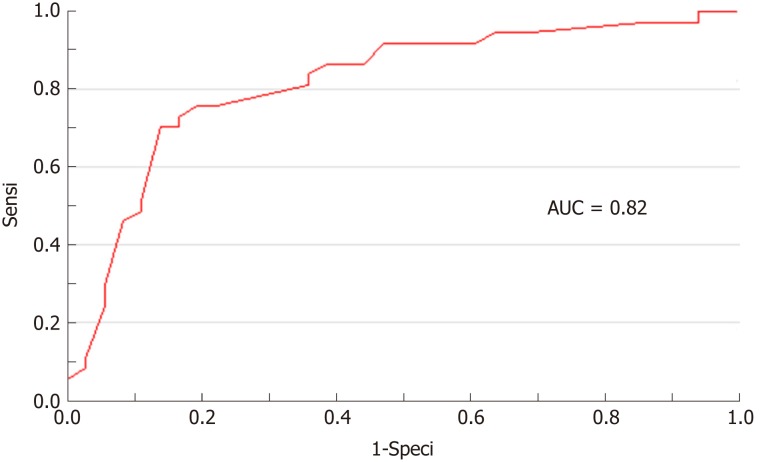
Results: Of the 367 patients, 73 patients with rectosigmoid endometriosis were evaluated by RS-EUS and underwent rectosigmoid surgery. After the univariate analysis was completed, thickness, width and infiltration of the submucosae were identified as potential predictive factors for bowel resection. In a multivariate logistic regression model, only thickness appeared to be a significant [odds ratio (OR) = 1.49, 95% confidence interval (CI): 1.04-2.12, P = 0.028] predictive factor for bowel resection. Receiver operating characteristic analysis performed showed that a thickness over 5.20 mm might be used as cut-off with a sensitivity of 76%, a specificity of 81%, and an area under carve = 0.82. The cut-off values for 100% sensitivity and 100% specificity were 0.90 mm and 10.00 mm, respectively. A trend concerning width to predict the need for resection was also observed (OR 1.12, 95%CI: 1.00-1.26, P = 0.054).
Conclusion: The presence of a rectosigmoid nodule of endometriosis greater than 5.20 mm thick on RS-EUS might predict the need for bowel resection.
Keywords: Bowel disease; Endometriosis; Endoscopy; Rectum and sigmoid; Surgery; Ultrasound.
Conflict of interest statement
Conflict-of-interest statement: We have no financial relationships to disclose.
Figures

References
-
- Giudice LC, Kao LC. Endometriosis. Lancet. 2004;364:1789–1799. - PubMed
-
- Williams TJ, Pratt JH. Endometriosis in 1,000 consecutive celiotomies: Incidence and management. Am J Obstet Gynecol. 1977;129:245–250. - PubMed
-
- Goncalves MO, Podgaec S, Dias JA, Jr, Gonzalez M, Abrao MS. Transvaginal ultrasonography with bowel preparation is able to predict the number of lesions and rectosigmoid layers affected in cases of deep endometriosis, defining surgical strategy. Hum Reprod. 2010;25:665–671. - PubMed
-
- Canon B, Collinet P, Piessen G, Rubod C. Résection rectale segmentaire et shaving rectal laparoscopiques pour endométriose: Morbidité péri-opératoire. Gynécologie Obstétrique Fertil. 2013;41:275–281. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
