

Global birth prevalence of congenital heart defects 1970-2017: updated systematic review and meta-analysis of 260 studies
- PMID: 30783674
- PMCID: PMC6469300
- DOI: 10.1093/ije/dyz009
Global birth prevalence of congenital heart defects 1970-2017: updated systematic review and meta-analysis of 260 studies
Abstract
Background: Globally, access to healthcare and diagnostic technologies are known to substantially impact the reported birth prevalence of congenital heart disease (CHD). Previous studies have shown marked heterogeneity between different regions, with a suggestion that CHD prevalence is rising globally, but the degree to which this reflects differences due to environmental or genetic risk factors, as opposed to improved detection, is uncertain. We performed an updated systematic review to address these issues.
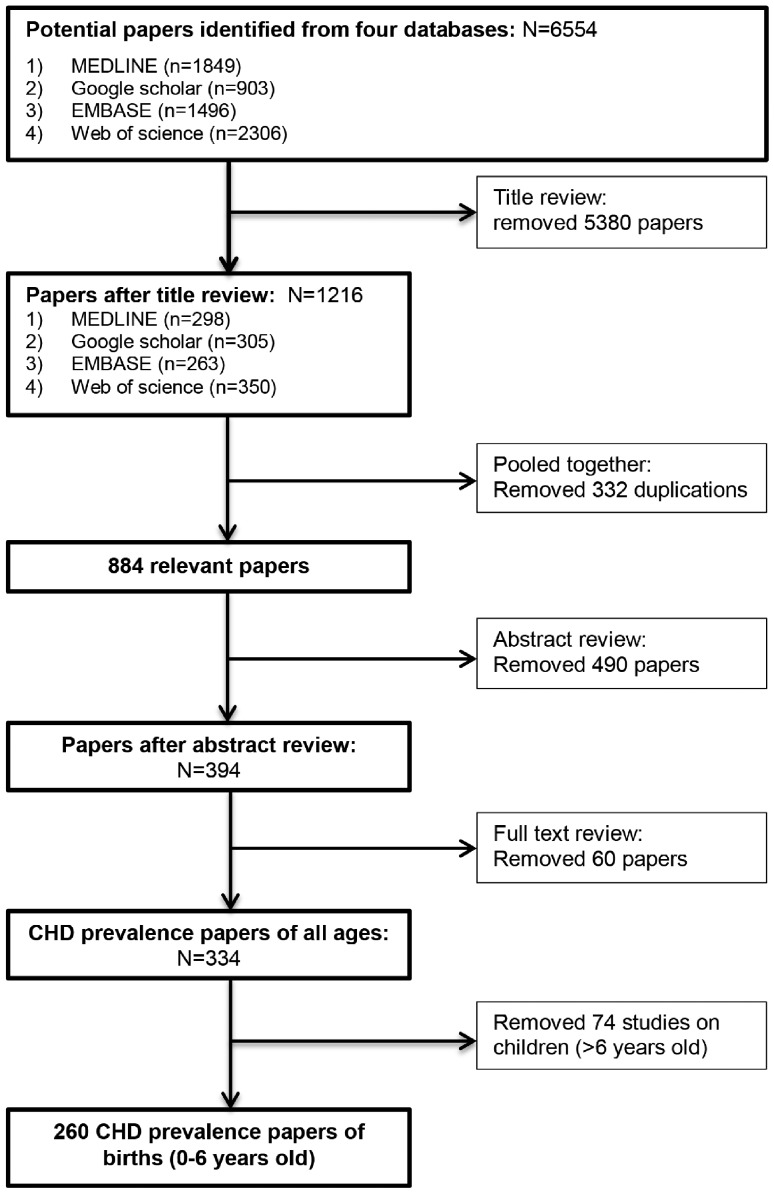
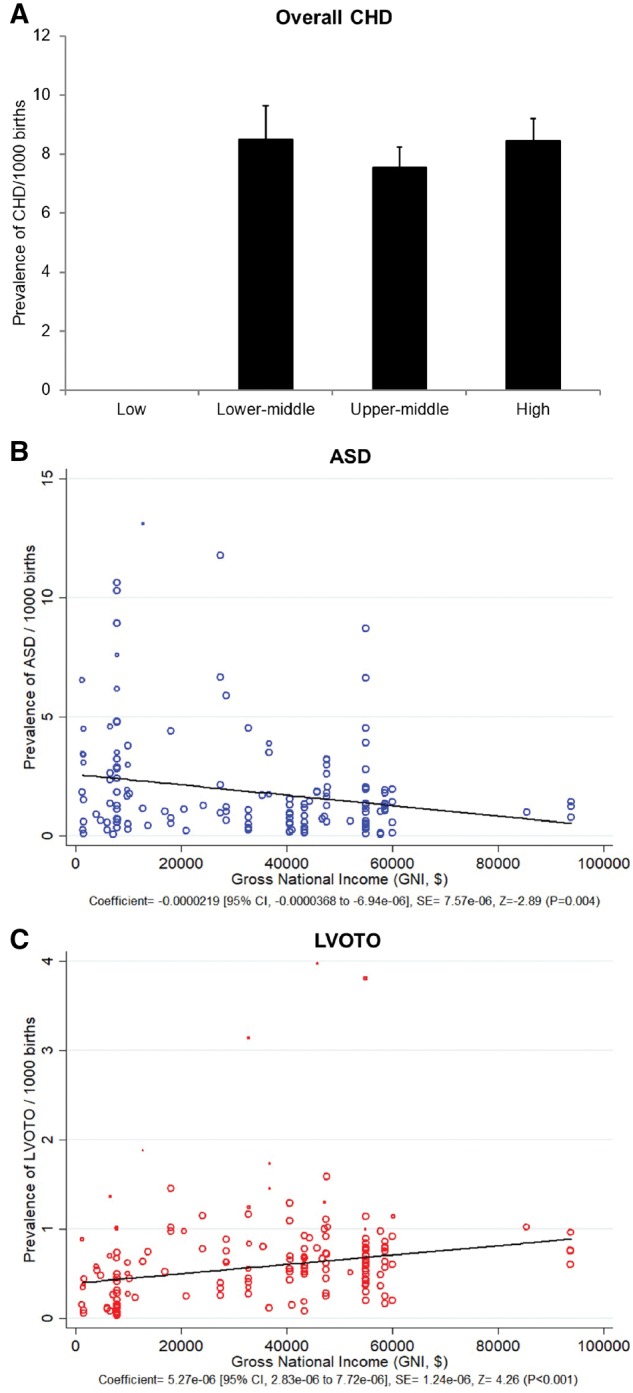
Methods: Studies reporting the birth prevalence of CHD between the years 1970-2017 were identified from searches of PubMed, EMBASE, Web of Science and Google Scholar. Data on the prevalence of total CHD and 27 anatomical subtypes of CHD were collected. Data were combined using random-effect models. Subgroup and meta-regression analyses were conducted, focused on geographical regions and levels of national income.
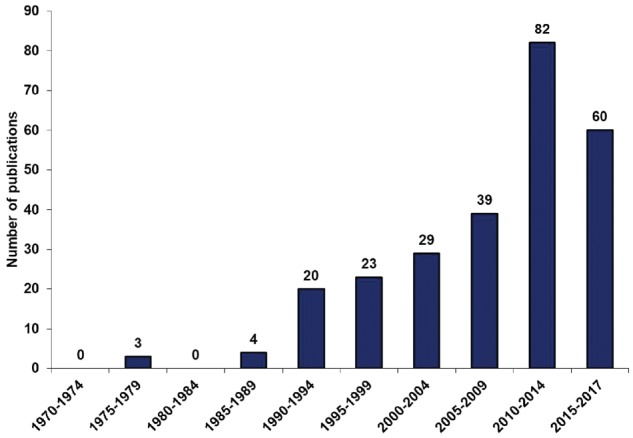
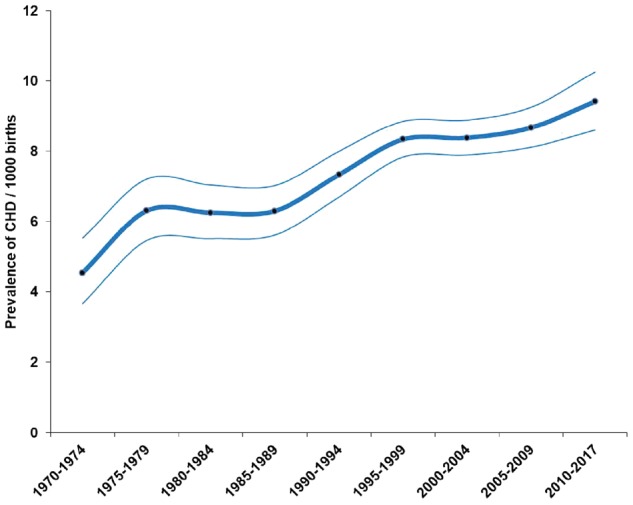
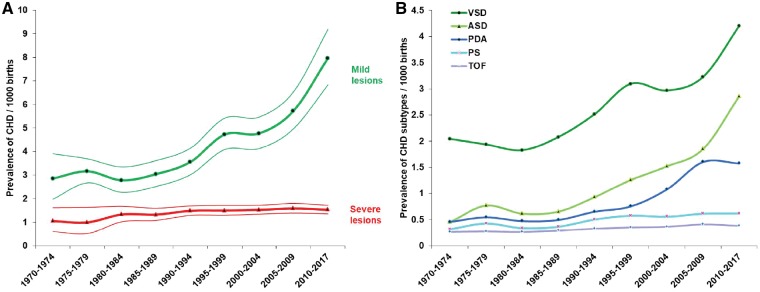
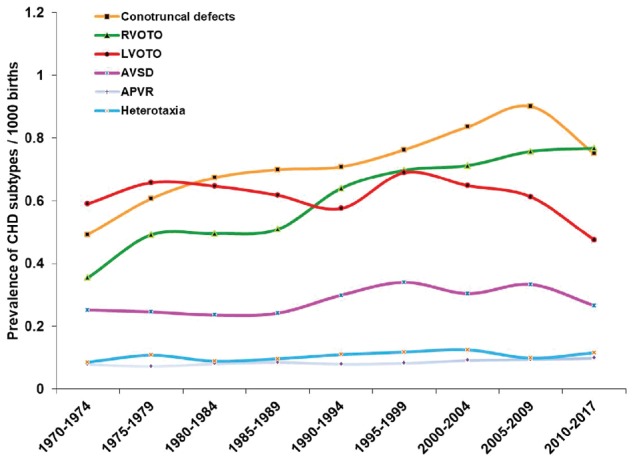
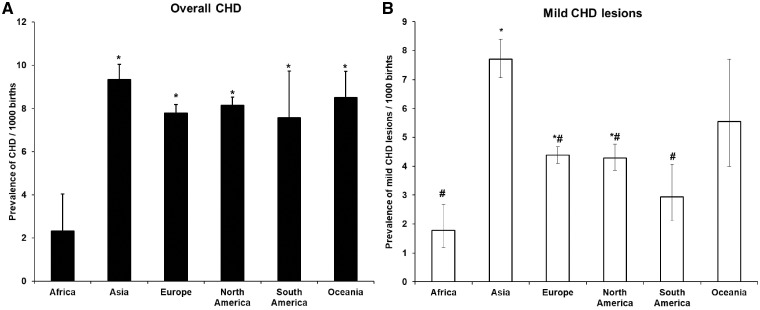
Results: Two hundred and sixty studies met the inclusion criteria, encompassing 130 758 851 live births. The birth prevalence of CHD from 1970-2017 progressively increased to a maximum in the period 2010-17 of 9.410/1000 [95% CI (confidence interval) 8.602-10.253]. This represented a significant increase over the fifteen prior years (P = 0.031). The change in prevalence of mild CHD lesions (ventricular septal defect, atrial septal defect and patent ductus arteriosus) together explained 93.4% of the increased overall prevalence, consistent with a major role of improved postnatal detection of less severe lesions. In contrast the prevalence of lesions grouped together as left ventricular outflow tract obstruction (which includes hypoplastic left heart syndrome) decreased from 0.689/1000 (95% CI 0.607-0.776) in 1995-99, to 0.475/1000 (95% CI 0.392-0.565; P = 0.004) in 2010-17, which would be consistent with improved prenatal detection and consequent termination of pregnancy when these very severe lesions are discovered. There was marked heterogeneity among geographical regions, with Africa reporting the lowest prevalence [2.315/1000 (95% CI 0.429-5.696)] and Asia the highest [9.342/1000 (95% CI 8.072-10.704)].
Conclusions: The reported prevalence of CHD globally continues to increase, with evidence of severe unmet diagnostic need in Africa. The recent prevalence of CHD in Asia for the first time appears higher than in Europe and America, where disease ascertainment is likely to be near-complete, suggesting higher genetic or environmental susceptibility to CHD among Asian people.
Keywords: Congenital heart disease; geographical region; meta-analysis; national income; prevalence; systematic review.
© The Author(s) 2019. Published by Oxford University Press on behalf of the International Epidemiological Association.
Figures
References
-
- van der Linde D, Konings EE, Slager MA et al. Birth prevalence of congenital heart disease worldwide: a systematic review and meta-analysis. J Am Coll Cardiol 2011;58:2241–7. - PubMed
-
- Blue GM, Kirk EP, Sholler GF, Harvey RP, Winlaw DS. Congenital heart disease: current knowledge about causes and inheritance. Med J Aust 2012;197:155–9. - PubMed
-
- Luchini C, Stubbs B, Solmi M, Veronese N. Assessing the quality of studies in meta-analyses: advantages and limitations of the Newcastle Ottawa Scale. World J Metaanal 2017;5:80–4.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
