

Clinical practice guideline for renal hypouricemia (1st edition)
- PMID: 30783949
- PMCID: PMC6437292
- DOI: 10.1007/s13577-019-00239-3
Clinical practice guideline for renal hypouricemia (1st edition)
Abstract
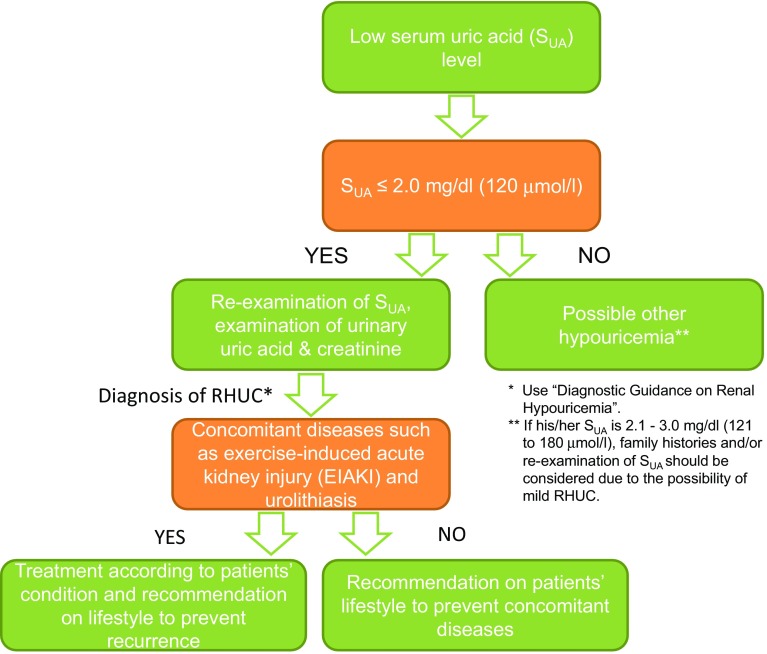
Renal hypouricemia (RHUC) is a disease caused by dysfunction of renal urate reabsorption transporters; however, diagnostic guidance and guidelines for RHUC have been lacking, partly due to the low evidence level of studies on RHUC. This review describes a world-first clinical practice guideline (CPG) and its first version in English for this condition. It was developed following the "MINDS Manual for Guideline Development" methodology, which prioritizes evidence-based medicine. It was published in Japanese in 2017 and later translated into English. The primary goal of this CPG is to clarify the criteria for diagnosing RHUC; another aim is to work towards a consensus on clinical decision-making. One of the CPG's unique points is that it contains textbook descriptions at the expert consensus level, in addition to two clinical questions and recommendations derived from a systematic review of the literature. The guidance shown in this CPG makes it easy to diagnose RHUC from simple blood and urine tests. This CPG contains almost all of the clinical foci of RHUC: epidemiology, pathophysiology, diagnostic guidance, clinical examinations, differential diagnosis, and complications, including exercise-induced acute kidney injury and urolithiasis. A CPG summary as well as a clinical algorithm to assist healthcare providers with a quick reference and notes from an athlete for both physicians and patients are included. We hope that this CPG will help healthcare providers and patients to make clinical decisions, and that it will promote further research on RHUC.
Keywords: Acute renal failure with severe loin pain and patchy renal ischemia after anaerobic exercise (ALPE); Clinical practice guideline (CPG); Evidence-based medicine (EBM); Exercise-induced acute kidney injury (EIAKI); Renal hypouricemia (RHUC).
Conflict of interest statement
The first author AN, and the corresponding author and the representative of the Guideline Development Committee Members NS declare that they have no conflicts of interest (COIs). Some of the other authors received lecture fees, research funds, scholarships or incentive donations from Teijin Pharma ltd, Sanwa Kagaku Kenkyusho Co., Ltd., Fujiyakuhin Co., Ltd, and Torii Pharmaceutical Co., Ltd. For the reported COIs shown above, the Guideline Developing Committee has devised measures to avoid the influence of their COIs regarding guideline development. See Supplementary Material for the detail of COIs and its counter measures.
Figures
References
-
- Akaoka I, Nishizawa T, Yano E, Takeuchi A, Nishida Y. Familial hypouricaemia due to renal tubular defect of urate transport. Ann Clin Res. 1975;7(5):318–324. - PubMed
Publication types
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
