

Incidence and prevalence of dementia associated with transient ischaemic attack and stroke: analysis of the population-based Oxford Vascular Study
- PMID: 30784556
- PMCID: PMC6390174
- DOI: 10.1016/S1474-4422(18)30442-3
Incidence and prevalence of dementia associated with transient ischaemic attack and stroke: analysis of the population-based Oxford Vascular Study
Abstract
Background: Risk of dementia after stroke is a major concern for patients and carers. Reliable data for risk of dementia, particularly after transient ischaemic attack or minor stroke, are scarce. We studied the risks of, and risk factors for, dementia before and after transient ischaemic attack and stroke.
Methods: The Oxford Vascular Study is a prospective incidence study of all vascular events in a population of 92 728 people residing in Oxfordshire, UK. Patients with transient ischaemic attack or stroke occurring between April 1, 2002, and March 31, 2012, were ascertained with multiple methods, including assessment in a dedicated daily emergency clinic and daily review of all hospital admissions. Pre-event and post-event (incident) dementia were diagnosed at initial assessment and during 5-years' follow-up on the basis of cognitive testing supplemented by data obtained from hand searches of all hospital and primary care records. We assessed the association between post-event dementia and stroke severity (as measured with the US National Institutes of Health Stroke Scale [NIHSS] score), location (ie, dysphasia), previous events, markers of susceptibility or reserve (age, low education, pre-morbid dependency, leucoaraiosis), baseline cognition, and vascular risk factors with Cox regression models adjusted for age, sex, and education. We compared incidence and prevalence of dementia in our population with published UK population age-matched and sex-matched rates.
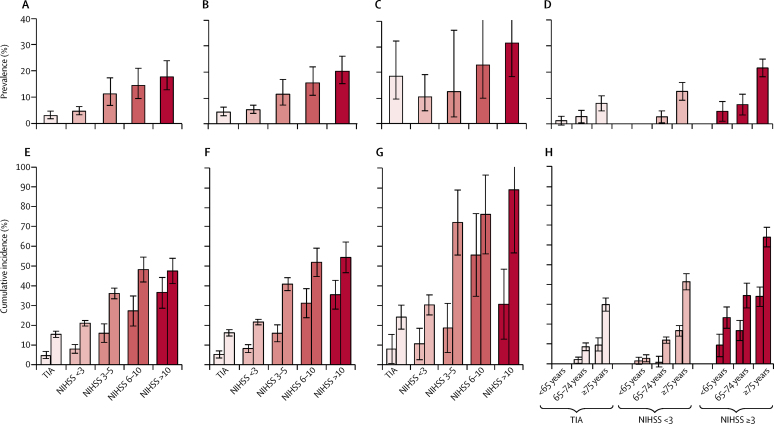
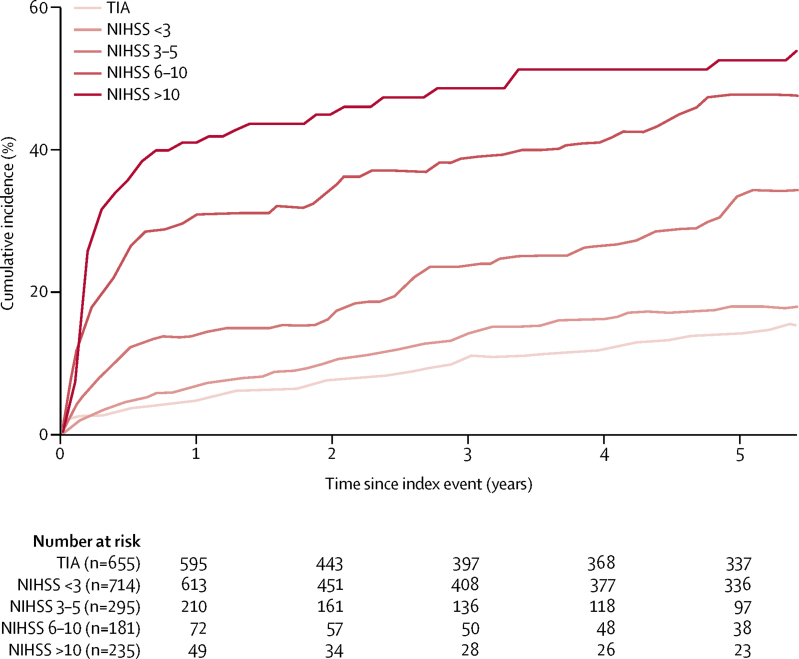
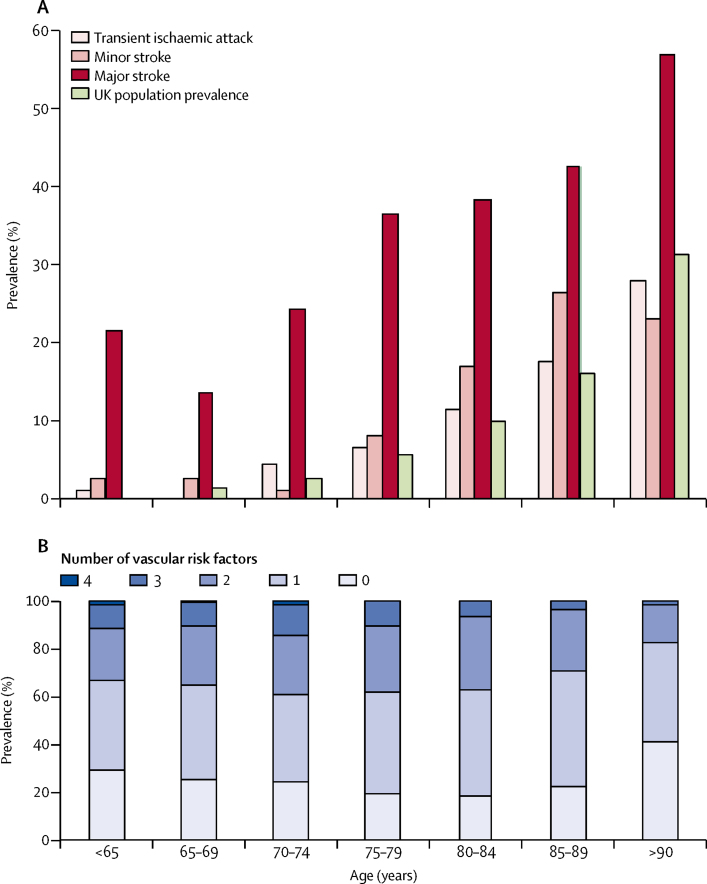
Findings: Among 2305 patients (mean age 74·4 years [SD 13·0]), 688 (30%) had transient ischaemic attacks and 1617 (70%) had strokes. Pre-event dementia was diagnosed in 225 patients; prevalence was highest in severe stroke (ie, NIHSS >10) and lowest in transient ischaemic attack. Of 2080 patients without pre-event dementia, 1982 (95%) were followed up to the end of study or death. Post-event dementia occurred in 432 of 2080 patients during 5 years of follow-up. The incidence of post-event dementia at 1 year was 34·4% (95% CI 29·7-41·5) in patients with severe stroke (NIHSS score >10), 8·2% (6·2-10·2) in those with minor stroke (NIHSS score <3), and 5·2% (3·4-7·0) in those with transient ischaemic attack. Compared with the UK age-matched and sex-matched population, the 1-year standardised morbidity ratio for the incidence of dementia was 47·3 (95% CI 35·9-61·2), 5·8 (4·4-7·5), and 3·5 (2·5-4·8), respectively. Consequently, prevalence of dementia in 1-year survivors was brought forward by approximately 25 years in those who had severe strokes, 4 years in those who had minor strokes, and 2 years in those who had transient ischaemic attacks. 5-year risk of dementia was associated with age, event severity, previous stroke, dysphasia, baseline cognition, low education, pre-morbid dependency, leucoaraiosis, and diabetes (p<0·0001 for all comparisons, except for previous stroke [p=0·006]).
Interpretation: The incidence of dementia in patients who have had a transient ischaemic attack or stroke varies substantially depending on clinical characteristics including lesion burden and susceptibility factors. Incidence of dementia is nearly 50 times higher in the year after a major stroke compared with that in the general population, but excess risk is substantially lower after transient ischaemic attack and minor stroke.
Funding: Wellcome Trust, Wolfson Foundation, British Heart Foundation, National Institute for Health Research, and the National Institute for Health Research Oxford Biomedical Research Centre.
Copyright © 2019 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Dementia risk after transient ischaemic attack and stroke.Lancet Neurol. 2019 Mar;18(3):223-225. doi: 10.1016/S1474-4422(18)30497-6. Epub 2019 Feb 12. Lancet Neurol. 2019. PMID: 30784546 No abstract available.
References
-
- Pendlebury ST, Rothwell PM. Prevalence, incidence, and factors associated with pre-stroke and post-stroke dementia: a systematic review and meta-analysis. Lancet Neurol. 2009;8:1006–1018. - PubMed
-
- Pendlebury ST. Dementia in patients hospitalized with stroke: rates, time course, and clinico-pathologic factors. Int J Stroke. 2012;7:570–581. - PubMed
-
- De Ronchi D, Palmer K, Pioggiosi P. The combined effect of age, education, and stroke on dementia and cognitive impairment on dementia in the elderly. Dement Geriatr Cogn Disord. 2007;24:266–273. - PubMed
-
- Kiphuth IC, Utz KS, Noble AJ, Köhrmann M, Schenk T. Increased prevalence of posttraumatic stress disorder in patients after transient ischemic attack. Stroke. 2014;45:3360–3366. - PubMed
-
- Pendlebury ST, Wadling S, Silver LE, Mehta Z, Rothwell PM. Transient cognitive impairment in TIA and minor stroke. Stroke. 2011;42:3116–3121. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
