

Effect of a novel vital sign device on maternal mortality and morbidity in low-resource settings: a pragmatic, stepped-wedge, cluster-randomised controlled trial
- PMID: 30784635
- PMCID: PMC6379820
- DOI: 10.1016/S2214-109X(18)30526-6
Effect of a novel vital sign device on maternal mortality and morbidity in low-resource settings: a pragmatic, stepped-wedge, cluster-randomised controlled trial
Abstract
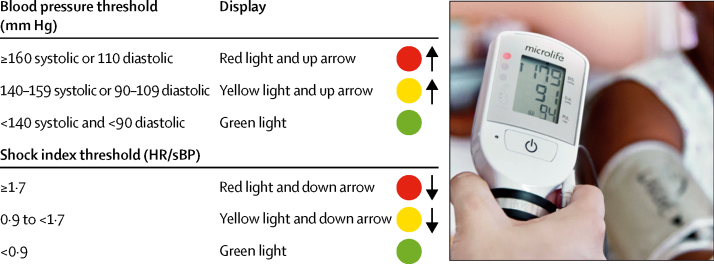
Background: In 2015, an estimated 303 000 women died in pregnancy and childbirth. Obstetric haemorrhage, sepsis, and hypertensive disorders of pregnancy account for more than 50% of maternal deaths worldwide. There are effective treatments for these pregnancy complications, but they require early detection by measurement of vital signs and timely administration to save lives. The primary aim of this trial was to determine whether implementation of the CRADLE Vital Sign Alert and an education package into community and facility maternity care in low-resource settings could reduce a composite of all-cause maternal mortality or major morbidity (eclampsia and hysterectomy).
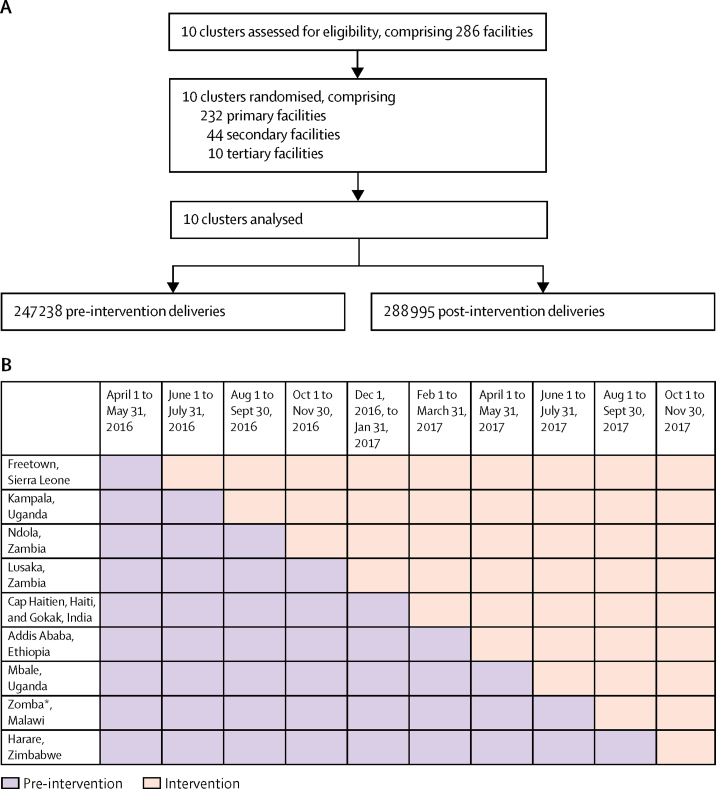
Methods: We did a pragmatic, stepped-wedge, cluster-randomised controlled trial in ten clusters across Africa, India, and Haiti, introducing the device into routine maternity care. Each cluster contained at least one secondary or tertiary hospital and their main referral facilities. Clusters crossed over from existing routine care to the CRADLE intervention in one of nine steps at 2-monthly intervals, with CRADLE devices replacing existing equipment at the randomly allocated timepoint. A computer-generated randomly allocated sequence determined the order in which the clusters received the intervention. Because of the nature of the intervention, this trial was not masked. Data were gathered monthly, with 20 time periods of 1 month. The primary composite outcome was at least one of eclampsia, emergency hysterectomy, and maternal death. This study is registered with the ISRCTN registry, number ISRCTN41244132.
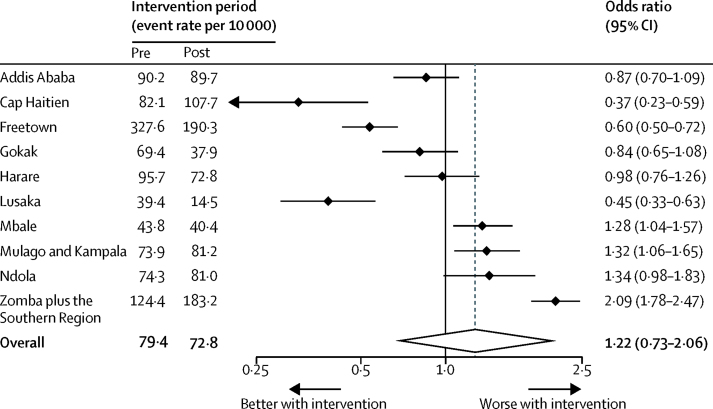
Findings: Between April 1, 2016, and Nov 30, 2017, among 536 223 deliveries, the primary outcome occurred in 4067 women, with 998 maternal deaths, 2692 eclampsia cases, and 681 hysterectomies. There was an 8% decrease in the primary outcome from 79·4 per 10 000 deliveries pre-intervention to 72·8 per 10 000 deliveries post-intervention (odds ratio [OR] 0·92, 95% CI 0·86-0·97; p=0·0056). After planned adjustments for variation in event rates between and within clusters over time, the unexpected degree of variability meant we were unable to judge the benefit or harms of the intervention (OR 1·22, 95% CI 0·73-2·06; p=0·45).
Interpretation: There was an absolute 8% reduction in primary outcome during the trial, with no change in resources or staffing, but this reduction could not be directly attributed to the intervention due to variability. We encountered unanticipated methodological challenges with this trial design, which can provide valuable learning for future research and inform the trial design of future international stepped-wedge trials.
Funding: Newton Fund Global Research Programme: UK Medical Research Council; Department of Biotechnology, Ministry of Science & Technology, Government of India; and UK Department of International Development.
Copyright © 2019 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
The challenge of measuring blood pressure in low-resource settings.Lancet Glob Health. 2019 Mar;7(3):e290-e291. doi: 10.1016/S2214-109X(19)30019-1. Lancet Glob Health. 2019. PMID: 30784622 No abstract available.
References
-
- WHO. UNICEF. UNFPA. The World Bank and the United Nations Population Division . World Health Organization; Geneva: 2015. Trends in maternal mortality: 1990 to 2015. Estimates by WHO, UNICEF, UNFPA, The World Bank and the United Nations Population Division.
-
- Say L, Chou D, Gemmill A. Global causes of maternal death: a WHO systematic analysis. Lancet Glob Health. 2014;2:e323–e333. - PubMed
-
- Campbell OMR, Graham WJ. Strategies for reducing maternal mortality: getting on with what works. Lancet. 2006;368:1284–1299. - PubMed
-
- Thaddeus S, Maine D. Too far to walk: maternal mortality in context. Soc Sci Med. 1994;38:1091–1110. - PubMed
-
- WHO . World Health Organization; Geneva: 2005. The World Health Report 2005: make every mother and child count. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
