

Cost-Effectiveness of Mitral Valve Repair Versus Replacement for Severe Ischemic Mitral Regurgitation: A Randomized Clinical Trial From the Cardiothoracic Surgical Trials Network
- PMID: 30785252
- PMCID: PMC6383805
- DOI: 10.1161/CIRCOUTCOMES.117.004466
Cost-Effectiveness of Mitral Valve Repair Versus Replacement for Severe Ischemic Mitral Regurgitation: A Randomized Clinical Trial From the Cardiothoracic Surgical Trials Network
Abstract
Background: The CTSN (Cardiothoracic Surgical Trials Network) recently reported no difference in left ventricular end-systolic volume index or in survival at 2 years between patients with severe ischemic mitral regurgitation (MR) randomized to mitral valve repair or replacement. However, replacement provided more durable correction of MR and fewer cardiovascular readmissions. Yet, costeffectiveness outcomes have not been addressed.
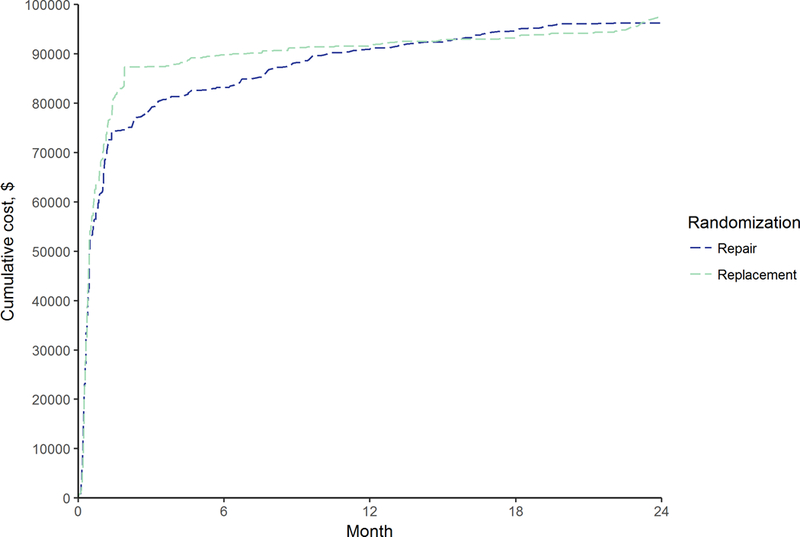
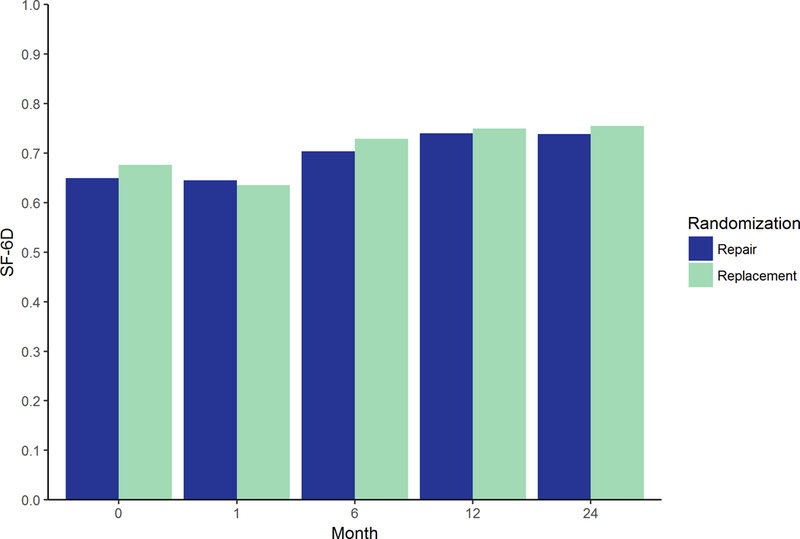
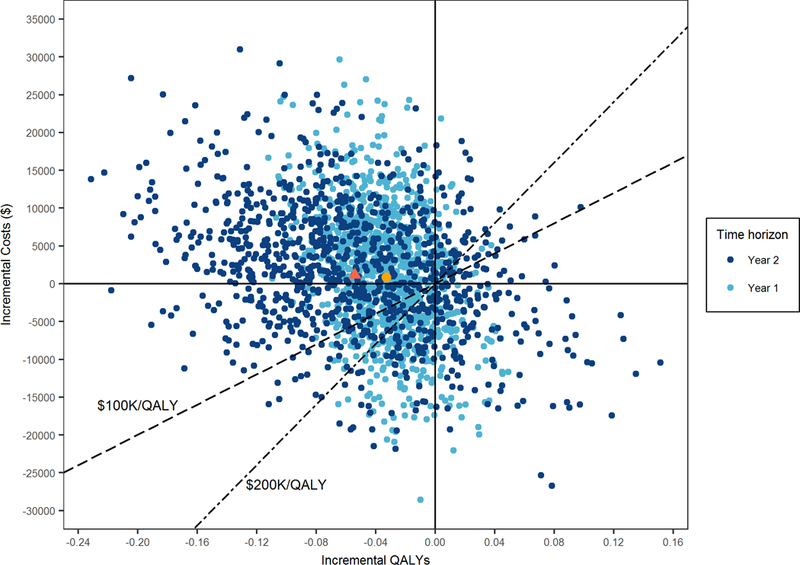
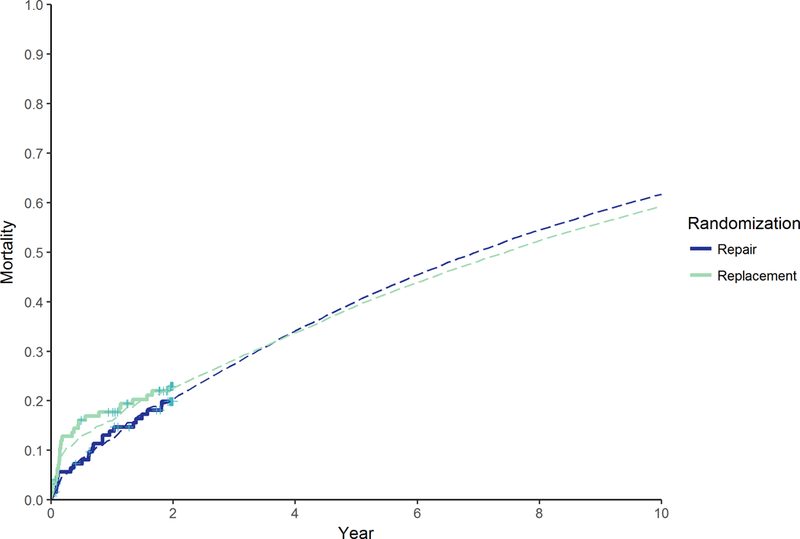
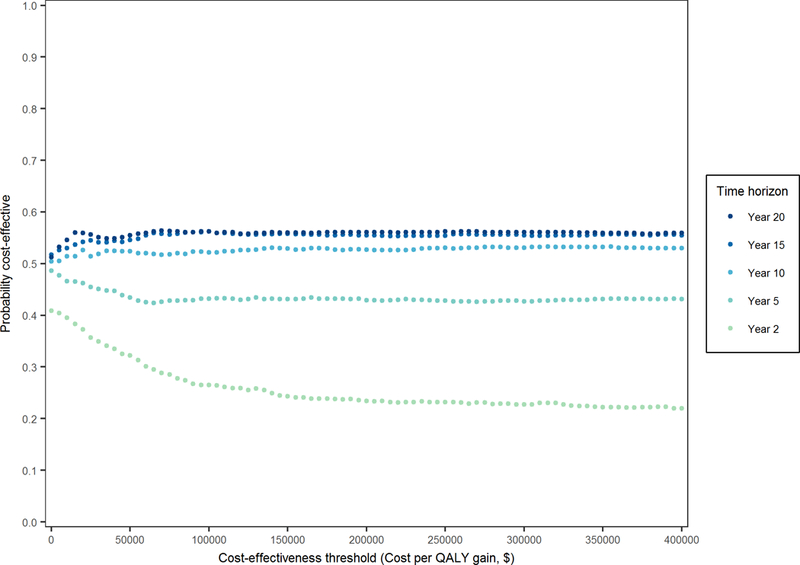
Methods and results: We conducted a cost-effectiveness analysis of the surgical treatment of ischemic MR based on the CTSN trial (n=126 for repair; n=125 for replacement). Patient-level data on readmissions, survival, qualityof- life, and US hospital costs were used to estimate costs and quality-adjusted life years per patient over the trial duration and a 10-year time horizon. We performed microsimulation for extrapolation of outcomes beyond the 2 years of trial data. Bootstrap and deterministic sensitivity analyses were done to address parameter uncertainty. In-hospital cost estimates were $78 216 for replacement versus $72 761 for repair (difference: $5455; 95% uncertainty interval [UI]: −7784–21 193) while 2-year costs were $97 427 versus $96 261 (difference: $1166; 95% UI: −16 253–17 172), respectively. Quality-adjusted life years at 2 years were 1.18 for replacement versus 1.23 for repair (difference: −0.05; 95% UI: −0.17 to 0.07). Over 5 and 10 years, the benefits of reduction in cardiovascular readmission rates with replacement increased, and survival minimally improved compared with repair. At 5 years, cumulative costs and quality-adjusted life years showed no difference on average, but by 10 years, there was a small, uncertain benefit for replacement: $118 023 versus $119 837 (difference: −$1814; 95% UI: −27 144 to 22 602) and qualityadjusted life years: 4.06 versus 3.97 (difference: 0.09; 95% UI: −0.87 to 1.08). After 10 years, the incremental cost-effectiveness of replacement continued to improve.
Conclusions: Our cost-effectiveness analysis predicts potential savings in cost and gains in quality-adjusted survival at 10 years when mitral valve replacement is compared with repair for severe ischemic MR. These projected benefits, however, were small and subject to variability. Efforts to further delineate predictors of long-term outcomes in patients with severe ischemic MR are needed to optimize surgical decisions for individual patients, which should yield more cost-effective care.
Clinical trial registration: URL: https://www.clinicaltrials.gov. Unique identifier: NCT00807040.
Keywords: Cardiac surgical procedures; cost-benefit analysis; health care costs; mitral valve; quality-adjusted life years.
2018 American Heart Association, Inc.
Conflict of interest statement
Dr Acker: consultant/advisory board for Thoratec (modest). Dr Gillinov: other research support from St. Jude Medical, Abbott (modest); consultant/advisory board for St. Jude Medical, Edwards Lifesciences (modest); consultant/advisory board for Abbott, Medtronic, CryoLife, AtriCure (significant). Dr Thourani: research grants from Edwards Lifesciences, Medtronic Corp, and Abbott Medical (modest); consultant/advisory board for Edwards Lifesciences, Abbott Medical (modest). Dr Robert L. Smith: research grant from Edwards Lifesciences (significant); speakers bureau for Abbott Medical (significant); consultant/advisory board for Abbott Medical, Edwards Lifesciences (significant); other from Abbott Medical, Edwards Lifesciences (significant). The other authors report no conflicts. This work was supported by a cooperative agreement (U01 HL088942) funded by the National Heart, Lung, and Blood Institute and the National Institute of Neurological Disorders and Stroke of the National Institute of Health and the Canadian Institutes of Health Research. Dr Ferket was supported by American Heart Association grant number 16MCPRP31030016. The views expressed in this article are those of the authors and do not necessarily represent the views of the National Heart, Lung, and Blood Institute; National Institutes of Health; or the United States Department of Health and Human Services.
Figures

Comment in
-
Replace or Repair?Circ Cardiovasc Qual Outcomes. 2018 Nov;11(11):e005093. doi: 10.1161/CIRCOUTCOMES.118.005093. Circ Cardiovasc Qual Outcomes. 2018. PMID: 30571341 No abstract available.
References
-
- Hillis GS, Moller JE, Pellikka PA, Bell MR, Casaclang-Verzosa GC and Oh JK. Prognostic significance of echocardiographically defined mitral regurgitation early after acute myocardial infarction. Am Heart J. 2005;150:1268–75. - PubMed
-
- Lamas GA, Mitchell GF, Flaker GC, Smith SC, Gersh BJ Jr, Basta L, Moye L, Braunwald E and Pfeffer MA. Clinical significance of mitral regurgitation after acute myocardial infarction. Survival and Ventricular Enlargement Investigators. Circulation. 1997;96:827–33. - PubMed
-
- Tcheng JE, Jackman JD, Nelson CL Jr, Gardner LH, Smith LR, Rankin JS, Califf RM and Stack RS. Outcome of patients sustaining acute ischemic mitral regurgitation during myocardial infarction. Ann Intern Med. 1992;117:18–24. - PubMed
-
- Schroder JN, Williams ML, Hata JA, Muhlbaier LH, Swaminathan M, Mathew JP, Glower DD, O’Connor CM, Smith PK and Milano CA. Impact of mitral valve regurgitation evaluated by intraoperative transesophageal echocardiography on long-term outcomes after coronary artery bypass grafting. Circulation. 2005;112:I293–8. - PubMed
-
- Barzilai B, Gessler C, Perez JE Jr, Schaab CandJaffe AS Significance of Doppler-detected mitral regurgitation in acute myocardial infarction. Am J Cardiol. 1988;61:220–3. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
