

First-Line Nivolumab Plus Ipilimumab in Advanced Non-Small-Cell Lung Cancer (CheckMate 568): Outcomes by Programmed Death Ligand 1 and Tumor Mutational Burden as Biomarkers
- PMID: 30785829
- PMCID: PMC6494267
- DOI: 10.1200/JCO.18.01042
First-Line Nivolumab Plus Ipilimumab in Advanced Non-Small-Cell Lung Cancer (CheckMate 568): Outcomes by Programmed Death Ligand 1 and Tumor Mutational Burden as Biomarkers
Abstract
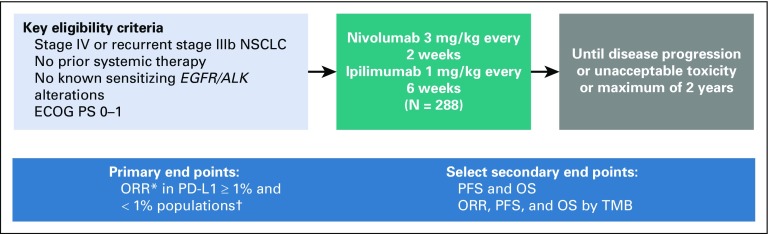
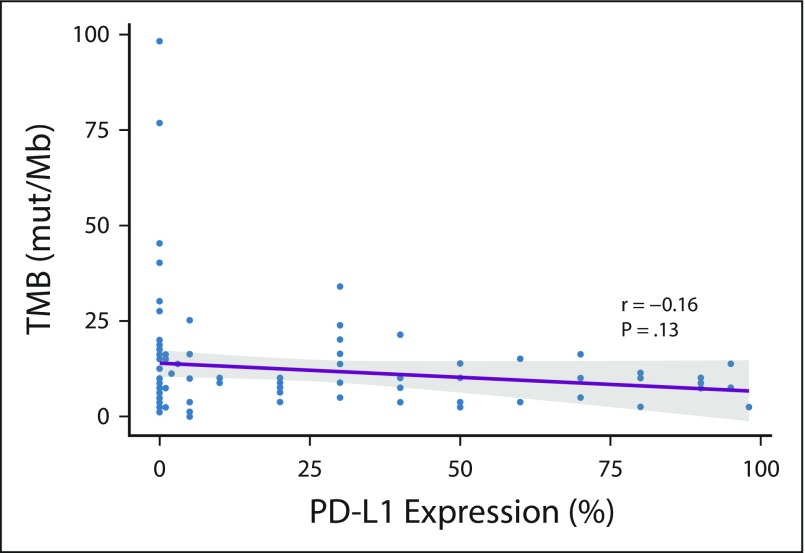
Purpose: CheckMate 568 is an open-label phase II trial that evaluated the efficacy and safety of nivolumab plus low-dose ipilimumab as first-line treatment of advanced/metastatic non-small-cell lung cancer (NSCLC). We assessed the association of efficacy with programmed death ligand 1 (PD-L1) expression and tumor mutational burden (TMB).
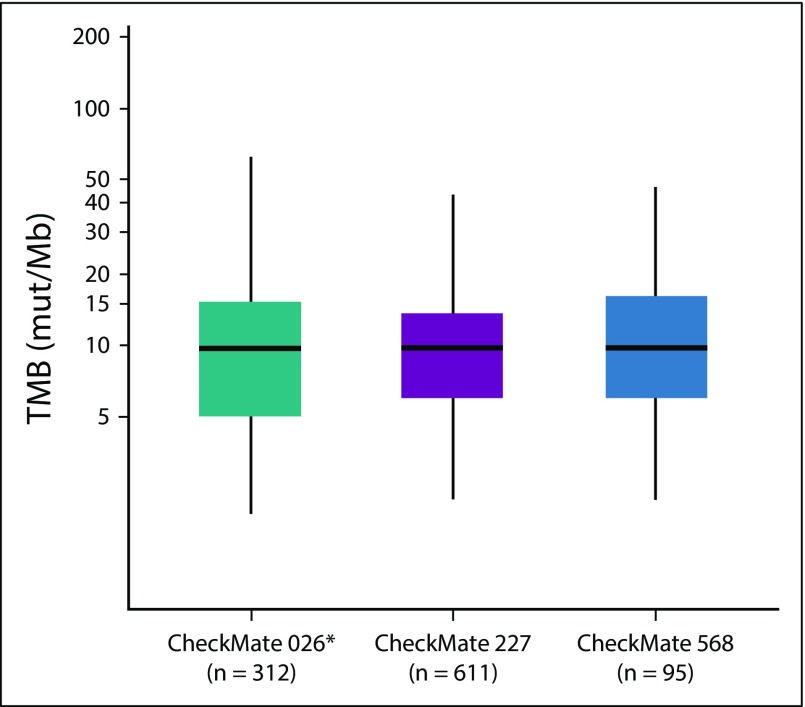
Patients and methods: Two hundred eighty-eight patients with previously untreated, recurrent stage IIIB/IV NSCLC received nivolumab 3 mg/kg every 2 weeks plus ipilimumab 1 mg/kg every 6 weeks. The primary end point was objective response rate (ORR) in patients with 1% or more and less than 1% tumor PD-L1 expression. Efficacy on the basis of TMB (FoundationOne CDx assay) was a secondary end point.
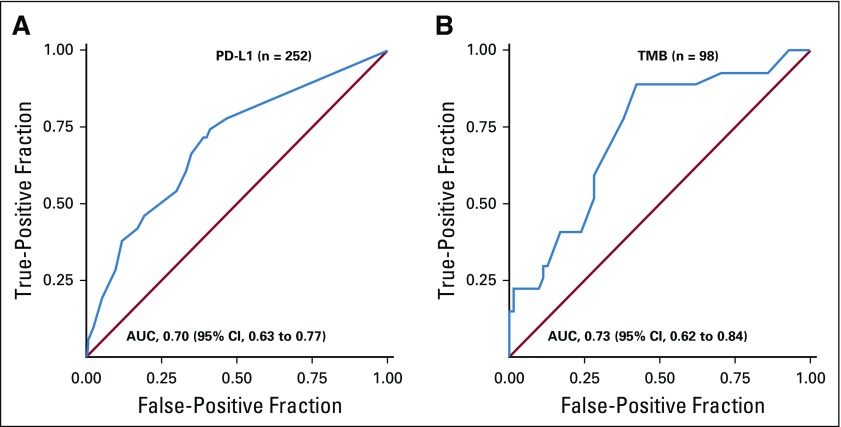
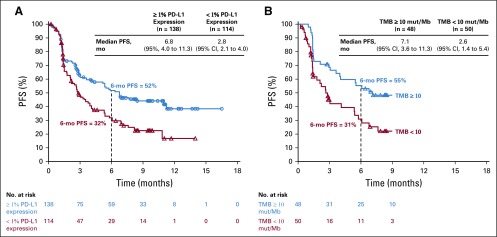
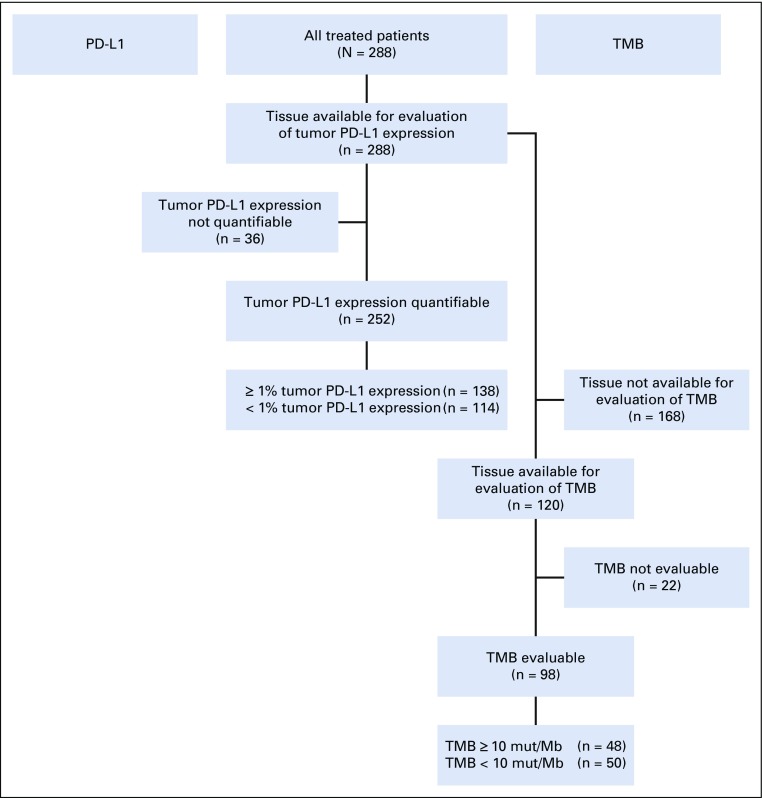
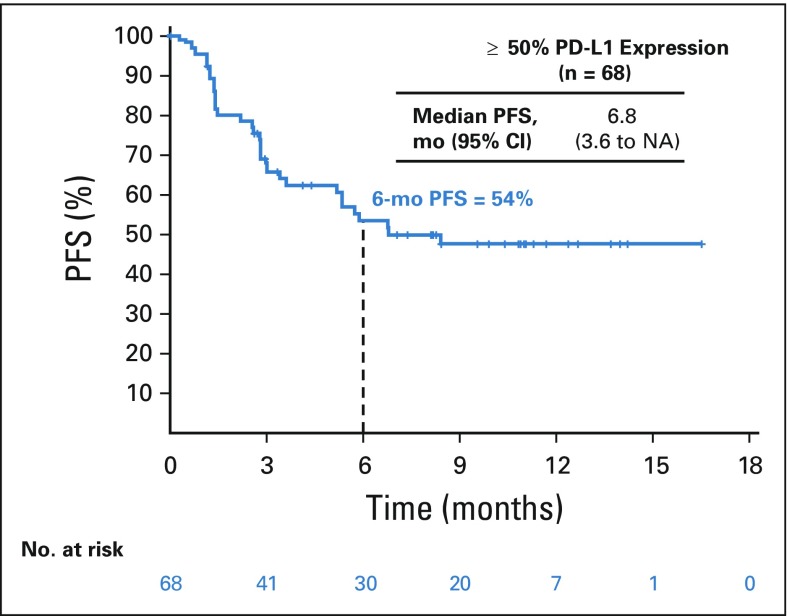
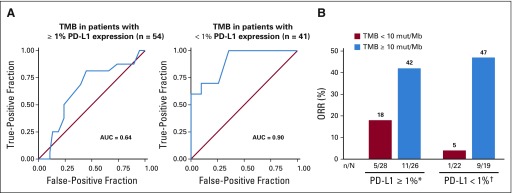
Results: Of treated patients with tumor available for testing, 252 patients (88%) of 288 were evaluable for PD-L1 expression and 98 patients (82%) of 120 for TMB. ORR was 30% overall and 41% and 15% in patients with 1% or greater and less than 1% tumor PD-L1 expression, respectively. ORR increased with higher TMB, plateauing at 10 or more mutations/megabase (mut/Mb). Regardless of PD-L1 expression, ORRs were higher in patients with TMB of 10 or more mut/Mb (n = 48: PD-L1, ≥ 1%, 48%; PD-L1, < 1%, 47%) versus TMB of fewer than 10 mut/Mb (n = 50: PD-L1, ≥ 1%, 18%; PD-L1, < 1%, 5%), and progression-free survival was longer in patients with TMB of 10 or more mut/Mb versus TMB of fewer than 10 mut/Mb (median, 7.1 v 2.6 months). Grade 3 to 4 treatment-related adverse events occurred in 29% of patients.
Conclusion: Nivolumab plus low-dose ipilimumab was effective and tolerable as a first-line treatment of advanced/metastatic NSCLC. TMB of 10 or more mut/Mb was associated with improved response and prolonged progression-free survival in both tumor PD-L1 expression 1% or greater and less than 1% subgroups and was thus identified as a potentially relevant cutoff in the assessment of TMB as a biomarker for first-line nivolumab plus ipilimumab.
Trial registration: ClinicalTrials.gov NCT02659059.
Figures

Comment in
-
PD-L1 positivity predicts response.Nat Rev Clin Oncol. 2019 Jun;16(6):337. doi: 10.1038/s41571-019-0199-z. Nat Rev Clin Oncol. 2019. PMID: 30846861 No abstract available.
References
-
- National Comprehensive Cancer Network NCCN guidelines: Non-small cell lung cancer. https://www.nccn.org/professionals/physician_gls/pdf/nscl.pdf
-
- Hanna N, Johnson D, Temin S, et al. Systemic therapy for stage IV non–small-cell lung cancer: American Society of Clinical Oncology Clinical Practice Guideline update. J Clin Oncol. 2017;35:3484–3515. - PubMed
-
- Keytruda (pembrolizumab) [package insert] Whitehouse Station, NJ: Merck & Co.; 2018.
-
- Opdivo (nivolumab) [package insert] Princeton, NJ: Bristol-Myers Squibb Company; 2018.
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
