

Diabetes Mellitus and Cardiovascular Disease
- PMID: 30786741
- PMCID: PMC6532416
- DOI: 10.1161/ATVBAHA.119.310961
Diabetes Mellitus and Cardiovascular Disease
Abstract
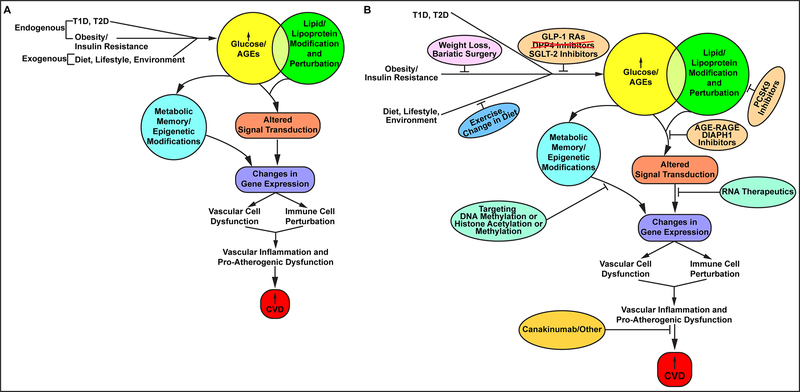
Cardiovascular disease remains a leading cause of morbidity and mortality in people with types 1 or 2 diabetes mellitus. Although beneficial roles for strict control of hyperglycemia have been suggested, such a strategy is not without liabilities. Specifically, the risk of hypoglycemia and its consequences remain an omnipresent threat with such approaches. The advent of the CVOT (Cardiovascular Outcomes Trials) for new antidiabetes mellitus treatments has uncovered unexpected benefits of cardiovascular protection in some of the new classes of agents, such as the GLP-1 RAs (glucagon-like peptide-1 receptor agonists) and the SGLT-2 (sodium-glucose cotransporter-2) inhibitors. Further, state-of-the-art approaches, such as antibodies to PCKSK9 (proprotein convertase subtilisin-kexin type 9); RNA therapeutics; agents targeting distinct components of the immune/inflammatory response; and novel small molecules that block the actions of RAGE (receptor for advanced glycation end products) signaling, also hold potential as new therapies for diabetes mellitus and cardiovascular disease. Finally, interventions such as weight loss, through bariatric surgery, may hold promise for benefit in diabetes and cardiovascular disease. In this Brief Review, some of the novel approaches and emerging targets for the treatment of diabetes mellitus and cardiovascular disease are discussed. Ultimately, identification of the optimal timing and combinations of such interventions, especially in the context of personalized approaches, together with emerging disease-modifying agents, holds great promise to reduce the burden that diabetes poses to the cardiovascular system.
Keywords: cardiovascular disease; diabetes mellitus; receptor for advanced glycation end products; therapeutics.
Figures
References
-
- Miller RG, Costacou T, Orchard TJ. Risk Factor Modeling for Cardiovascular Disease in Type I Diabetes in the Pittsburgh Epidemiology of Diabetes Complications (EDC) Study: A Comparison to the Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications Study. Diabetes. 2018 - PMC - PubMed
-
- Rawshani A, Rawshani A, Franzen S, Sattar N, Eliasson B, Svensson AM, Zethelius B, Miftaraj M, McGuire DK, Rosengren A, Gudbjornsdottir S. Risk Factors, Mortality, and Cardiovascular Outcomes in Patients with Type 2 Diabetes. N Engl J Med. 2018;379:633–644 - PubMed
