

Serious adverse events and lifetime risk of reoperation after elective shoulder replacement: population based cohort study using hospital episode statistics for England
- PMID: 30786996
- PMCID: PMC6380386
- DOI: 10.1136/bmj.l298
Serious adverse events and lifetime risk of reoperation after elective shoulder replacement: population based cohort study using hospital episode statistics for England
Abstract
Objectives: To provide accurate risk estimates of serious adverse events after elective shoulder replacement surgery for arthritis, including age and sex specific estimates of the lifetime risk of revision surgery.
Design: Population based cohort study.
Setting: Hospital episode statistics for NHS England, including civil registration mortality data.
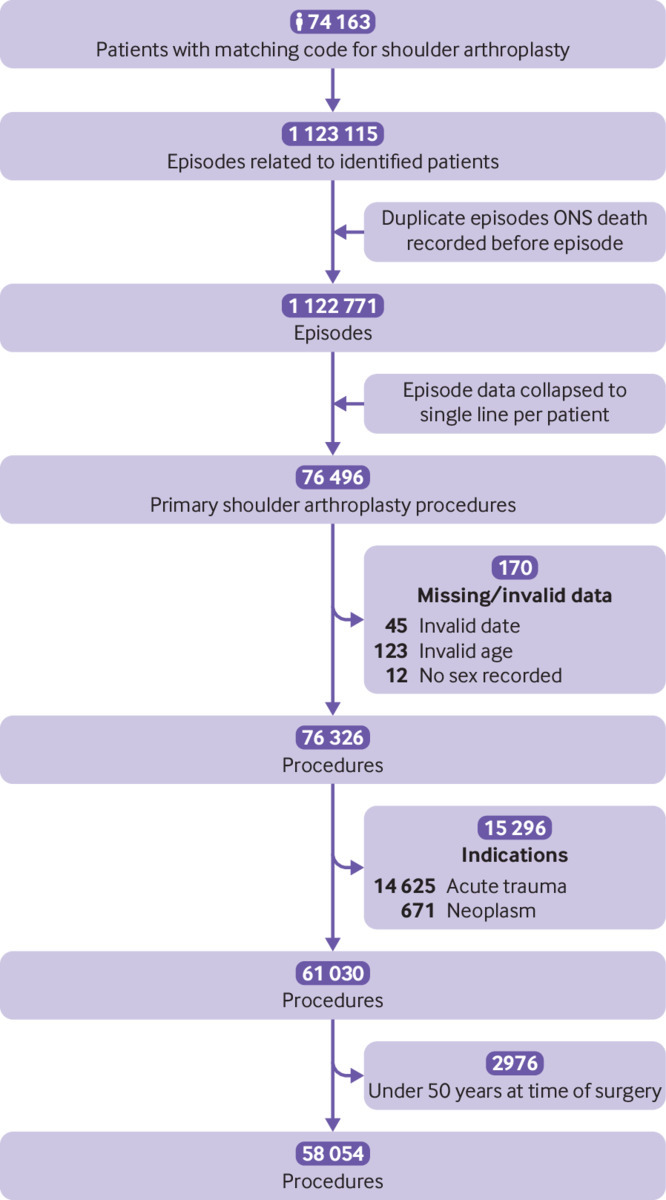
Participants: 58 054 elective shoulder replacements in 51 895 adults (aged ≥50 years) between April 1998 and April 2017.
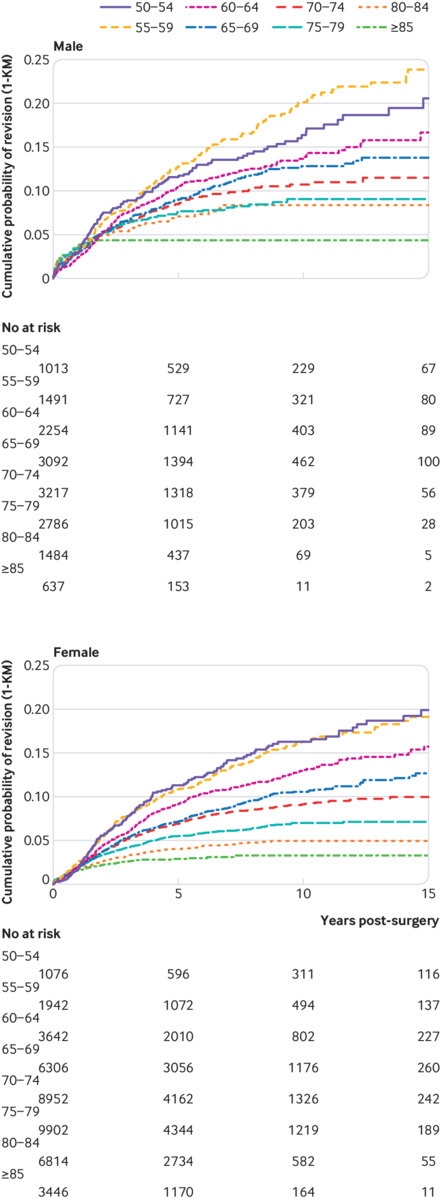
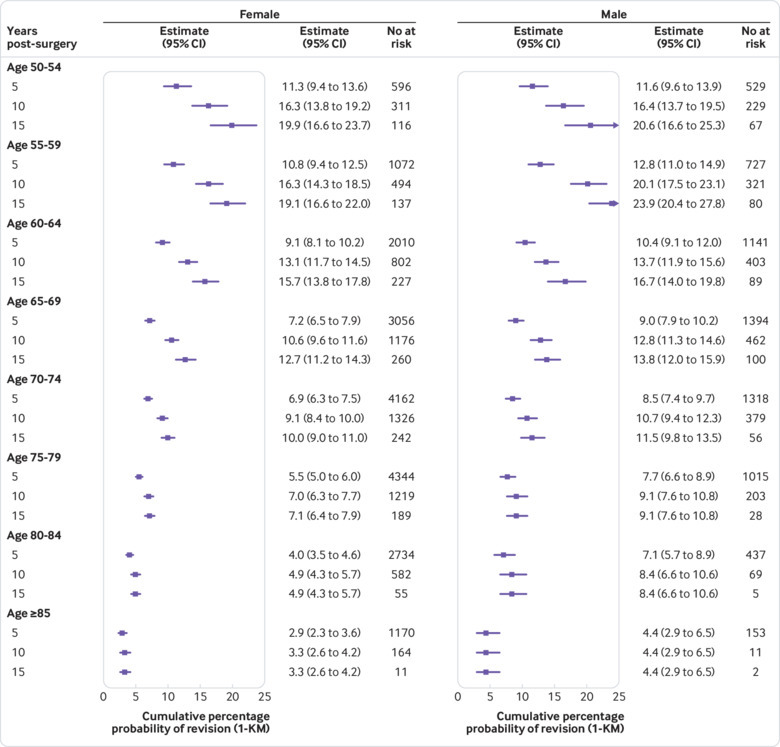
Main outcome measures: The lifetime risk of revision surgery, calculated using an actuarial life table approach and the cumulative probability method. Rates of serious adverse events at 30 and 90 days post-surgery: pulmonary embolism, myocardial infarction, lower respiratory tract infection, acute kidney injury, urinary tract infection, cerebrovascular events, and all cause death. Secondary outcome measures were the number of surgeries performed each year and Kaplan-Meier estimates of revision risk at 3, 5, 10, and 15 years.
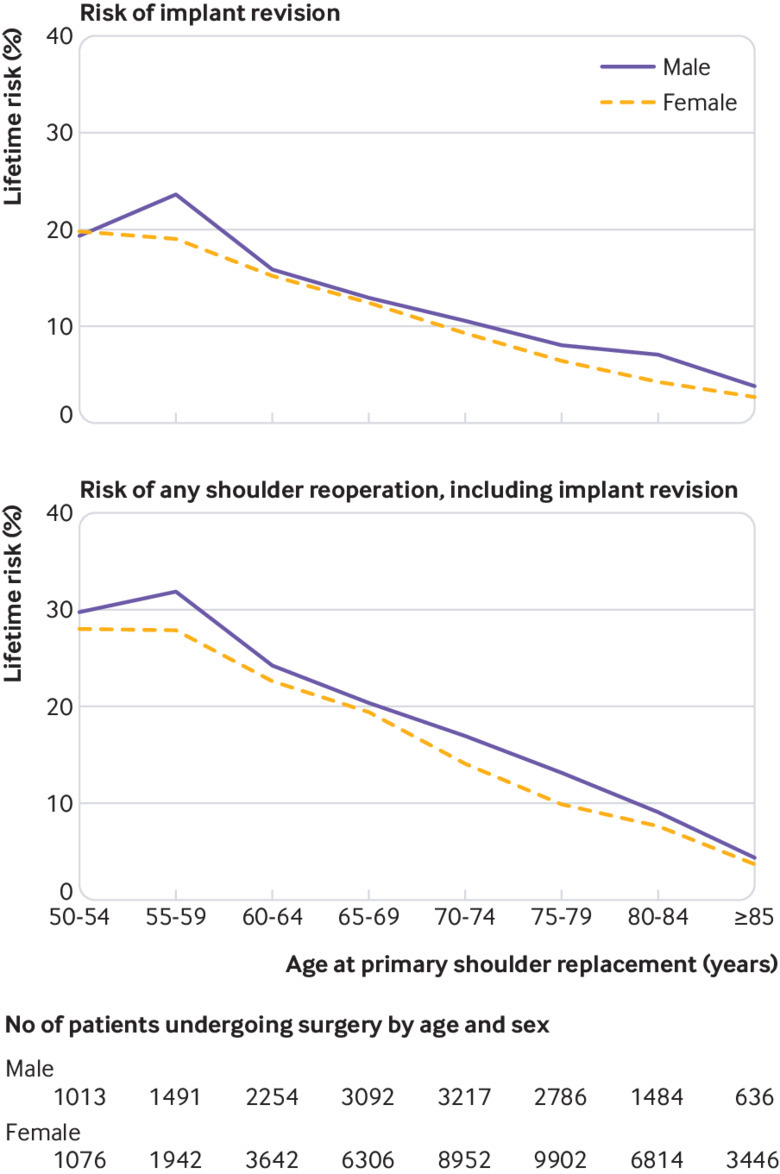
Results: The number of shoulder replacements performed each year increased 5.6-fold between 1998 and 2017. Lifetime risks of revision surgery ranged from 1 in 37 (2.7%, 95% confidence interval 2.6% to 2.8%) in women aged 85 years and older to 1 in 4 (23.6%, 23.2% to 24.0%) in men aged 55-59 years. The risks of revision were highest during the first five years after surgery. The risk of any serious adverse event at 30 days post-surgery was 1 in 28 (3.5%, 3.4% to 3.7%), and at 90 days post-surgery was 1 in 22 (4.6%, 4.4% to 4.8%). At 30 days, the relative risk of pulmonary embolism compared with baseline population risk was 61 (95% confidence interval 50 to 73) for women aged 50-64. Serious adverse events were associated with increasing age, comorbidity, and male sex. 1 in 5 (21.2%, 17.9% to 25.1%) men aged 85 years and older experienced at least one serious adverse event within 90 days.
Conclusions: Younger patients, particularly men, need to be aware of a higher likelihood of early failure of shoulder replacement and the need for further and more complex revision replacement surgery. All patients should be counselled about the risks of serious adverse events. These risks are higher than previously considered, and for some could outweigh any potential benefits. Our findings caution against unchecked expansion of shoulder replacement surgery in both younger and older patients. The more accurate age and sex specific estimates of risk from this study are long overdue and should improve shared decision making between patients and clinicians.
Study registration: ClinicalTrials.gov NCT03573765.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: no support from any organisation for the submitted work other than that listed above; no other financial relationships with organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Figures
References
-
- Fevang B-TS, Lygre SHL, Bertelsen G, Skredderstuen A, Havelin LI, Furnes O. Pain and function in eight hundred and fifty nine patients comparing shoulder hemiprostheses, resurfacing prostheses, reversed total and conventional total prostheses. Int Orthop 2013;37:59-66. 10.1007/s00264-012-1722-3. - DOI - PMC - PubMed
-
- Boorman RS, Kopjar B, Fehringer E, Churchill RS, Smith K, Matsen FA., 3rd The effect of total shoulder arthroplasty on self-assessed health status is comparable to that of total hip arthroplasty and coronary artery bypass grafting. J Shoulder Elbow Surg 2003;12:158-63. 10.1067/mse.2003.18. - DOI - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous