

Gastrointestinal stromal tumors: a comprehensive review
- PMID: 30788170
- PMCID: PMC6351301
- DOI: 10.21037/jgo.2018.08.20
Gastrointestinal stromal tumors: a comprehensive review
Abstract
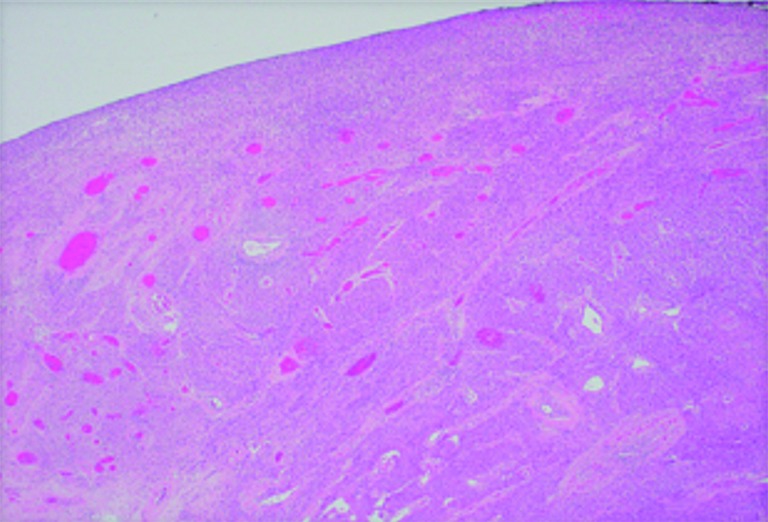
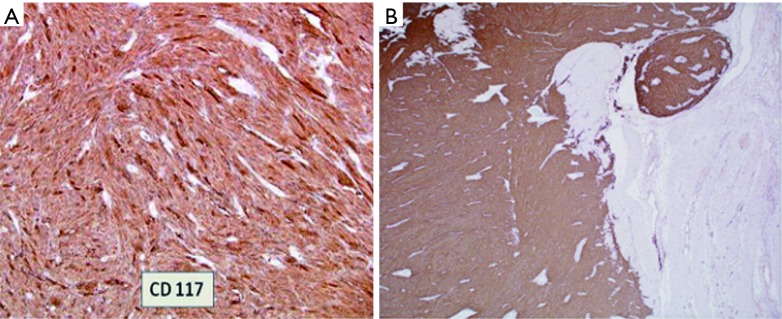
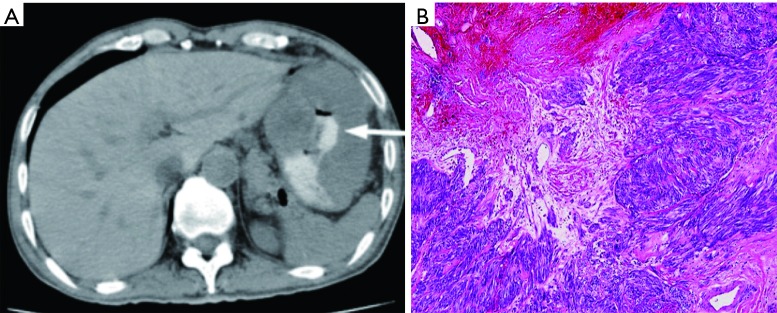
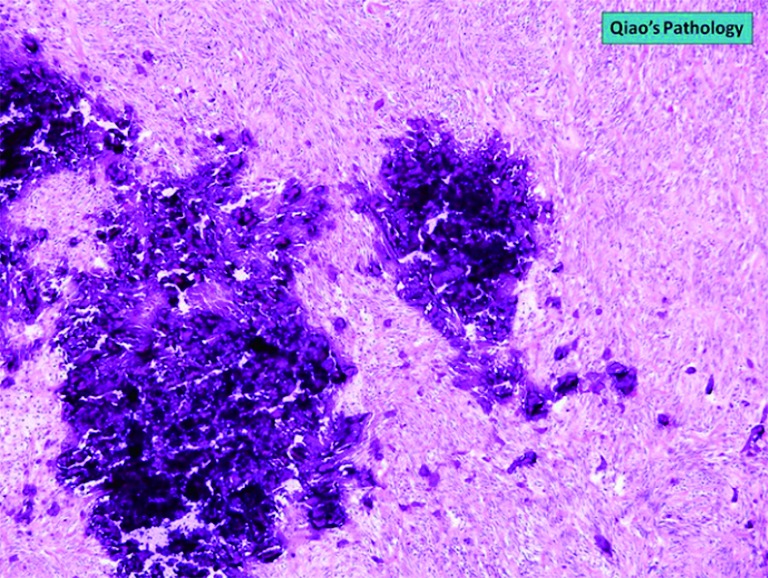
Gastrointestinal stromal tumors (GISTs) are rare neoplasms of the gastrointestinal tract associated with high rates of malignant transformation. Most GISTs present asymptomatically. They are best identified by computed tomography (CT) scan and most stain positive for CD117 (C-Kit), CD34, and/or DOG-1. There have been many risk stratification classifications systems which are calculated based on tumor size, mitotic rate, location, and perforation. The approaches to treating GISTs are to resect primary low-risk tumors, resect high-risk primary or metastatic tumors with imatinib 400 mg daily for 12 months, or if the tumor is unresectable, neoadjuvant imatinib 400 mg daily followed by surgical resection is recommended. Sunitinib is required for KIT exon 9, 13, and 14 mutations, while ponatinib is used for exon 17 mutations and regorafenib for highly refractory tumors. High-risk tumors should be monitored for recurrence with serial abdominal CT scans. Radiofrequency ablation has shown to be effective when surgery is not suitable. Newer therapies of ipilimumab, nivolumab, and endoscopic ultrasound alcohol ablation have shown promising results. This report addresses the epidemiology, clinical presentation, diagnostic imaging, histologic diagnosis, classification and risk stratification, staging and grading, surgical treatment, adjuvant treatment, and metastasis of GISTs.
Keywords: Gastrointestinal stromal tumor (GIST); outcome; prognosis; risk classification; tyrosine kinase receptor inhibitor (TKI).
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures


References
Publication types
LinkOut - more resources
Full Text Sources