

Patient-specific 3D printed pulmonary artery model with simulation of peripheral pulmonary embolism for developing optimal computed tomography pulmonary angiography protocols
- PMID: 30788248
- PMCID: PMC6351806
- DOI: 10.21037/qims.2018.10.13
Patient-specific 3D printed pulmonary artery model with simulation of peripheral pulmonary embolism for developing optimal computed tomography pulmonary angiography protocols
Abstract
Background: Computed tomography pulmonary angiography (CTPA) is the preferred imaging modality for diagnosis of patients with suspected pulmonary embolism (PE). Radiation dose associated with CTPA has been significantly reduced due to the use of dose-reduction strategies, however, investigation of low-dose CTPA with use of different kVp and pitch values has not been systematically studied. The aim of this study was to utilize a 3D printed pulmonary model with simulation of small thrombus in the pulmonary arteries for development of optimal CTPA protocols.
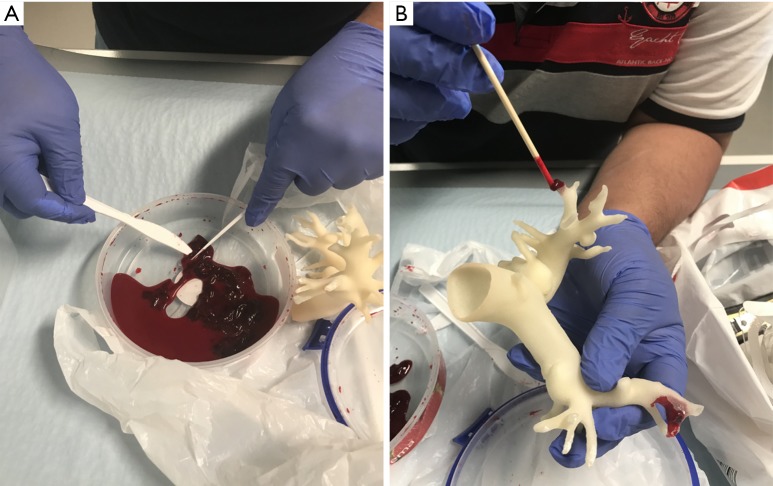
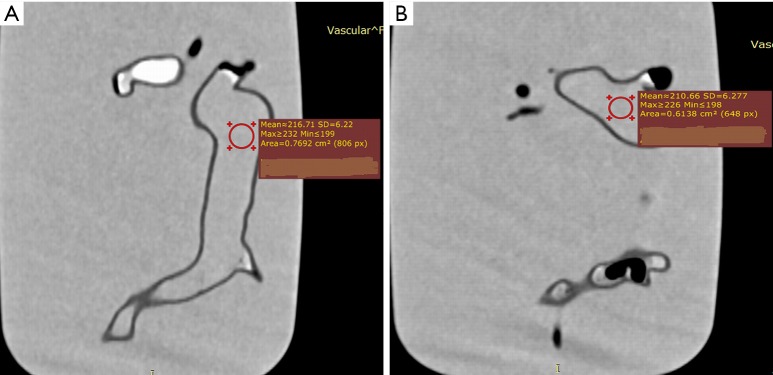
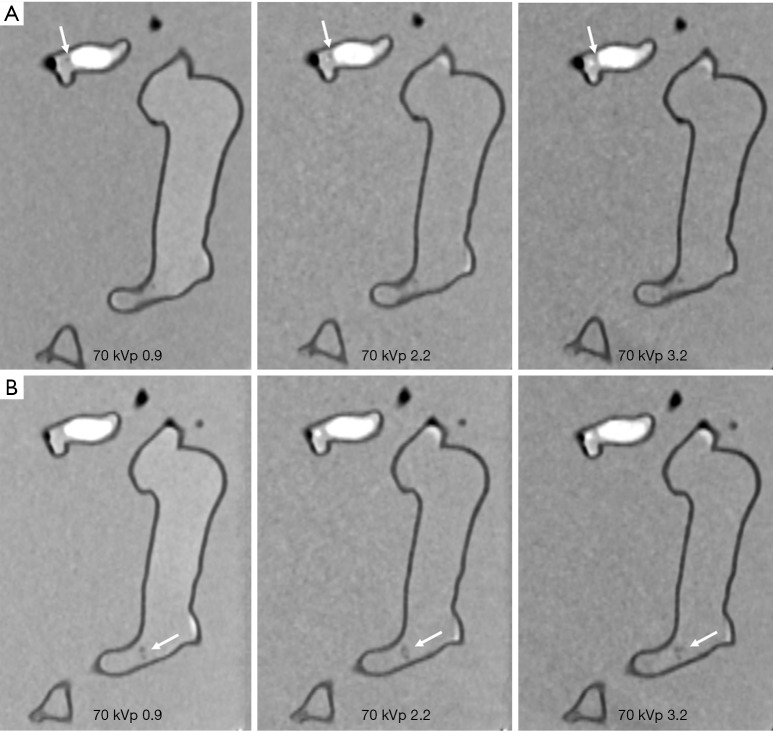
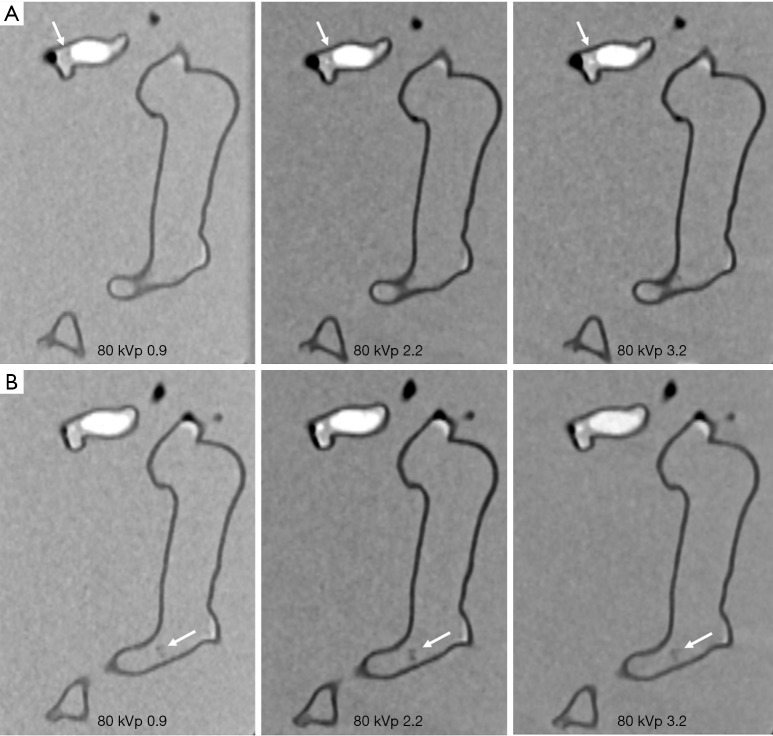
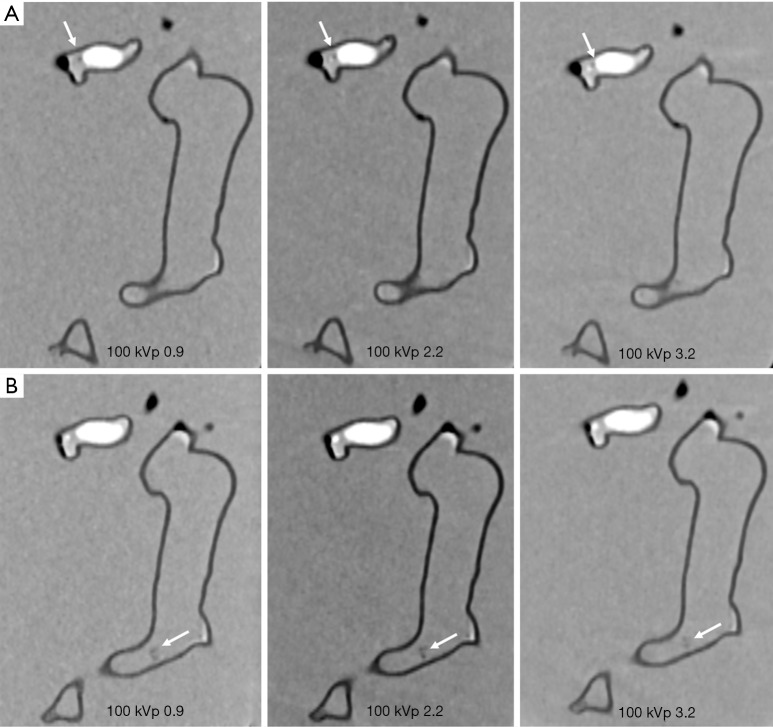
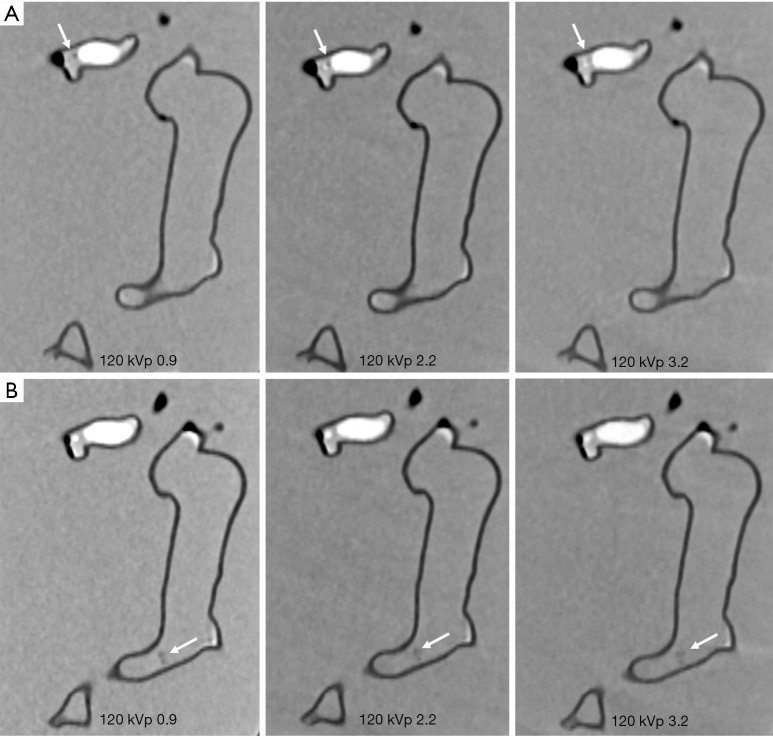
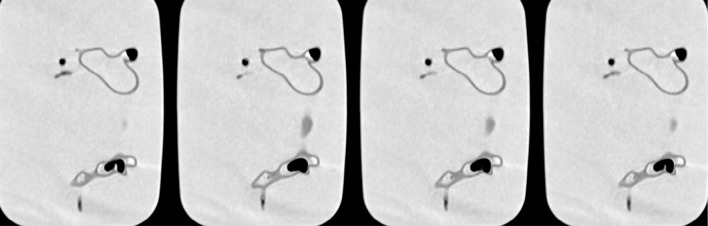
Methods: Animal blood clots were inserted into the pulmonary arteries to simulate peripheral embolism based on a realistic 3D printed pulmonary artery model. The 3D printed model was scanned with 192-slice 3rd generation dual-source CT with 1 mm slice thickness and 0.5 mm reconstruction interval. All images were reconstructed with advanced modelled iterative reconstruction (IR) at a strength level of 3. CTPA scanning parameters were as follows: 70, 80, 100 and 120 kVp, 0.9, 2.2 and 3.2 pitch values. Quantitative assessment of image quality was determined by measuring signal-to-noise ratio (SNR) in both main pulmonary arteries, while qualitative analysis of images was scored by two experienced radiologists (score of 1 indicates poor visualization of thrombus with no confidence, and score of 5 excellent visualization of thrombus with high confidence) to determine the image quality in relation to different scanning protocols for detection of thrombus in the pulmonary arteries.
Results: No significant differences were found in SNR measurements among all CTPA protocols (P>0.05), regardless of kVp or pitch values used, although SNR was higher with 120 kVp and 0.9 and 2.2 pitch protocols than that in other protocols. The thrombi were detected in all images, with 70 kVp and 3.2 pitch protocol scored the lowest with a score of 3 by two observers, and images with other protocols were scored 4 or 5. Lowering kVp from 120 to 70 with use of high-pitch 2.2 or 3.2 protocol resulted in up to 80% dose reduction without significantly affecting image quality.
Conclusions: Low-dose CT pulmonary angiography protocols comprising 70 kVp and high pitch 2.2 or 3.2 allow for detection of peripheral PE with significant reduction in radiation dose while images are still considered diagnostic.
Keywords: Assessment; computed tomography pulmonary angiography (CTPA); optimization; pitch; pulmonary embolism (PE); reduction; three-dimensional printing.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures

References
-
- Sun Z, Lei J. Diagnostic yield of CT pulmonary angiography in the diagnosis of pulmonary embolism: a single center experience. Interv Cardiol 2017;9:191-8. 10.4172/Interventional-Cardiology.1000577 - DOI
LinkOut - more resources
Full Text Sources
Miscellaneous