

Genetic Drivers of Pancreatic Cancer Are Identical Between the Primary Tumor and a Secondary Lesion in a Long-Term (>5 Years) Survivor After a Whipple Procedure
- PMID: 30788462
- PMCID: PMC6371588
- DOI: 10.1089/pancan.2018.0015
Genetic Drivers of Pancreatic Cancer Are Identical Between the Primary Tumor and a Secondary Lesion in a Long-Term (>5 Years) Survivor After a Whipple Procedure
Abstract
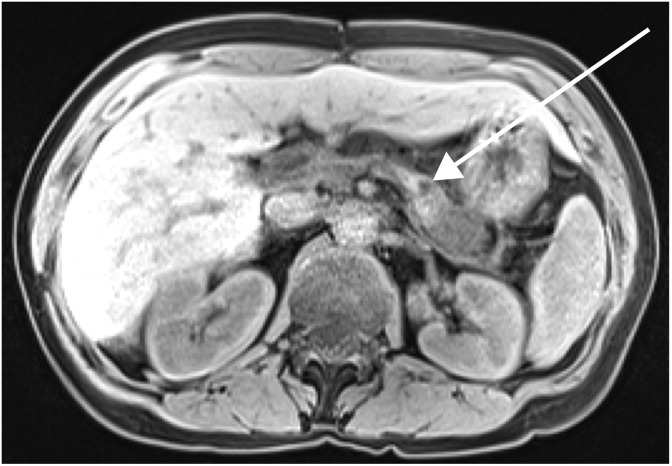
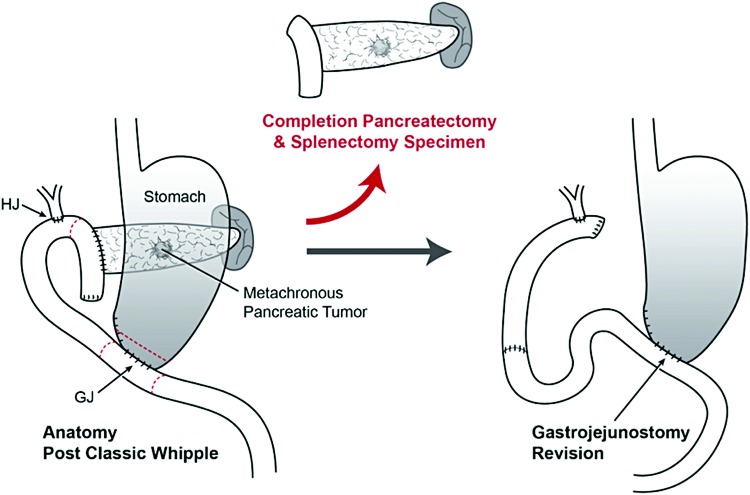
Background: A new mass in the remnant pancreas of a patient with previously resected pancreatic ductal adenocarcinoma (PDA) typically represents either a recurrence of the initial primary tumor or a second primary tumor. Recent advances in next-generation sequencing (NGS) strategies allow us to compare the genetic makeup of primary and secondary lesions. Case presentation: A 50-year-old Caucasian female presented for a surgical evaluation of a new biopsy-proven PDA at the junction of the body and tail of the pancreas. Six years prior, in 2011, the patient was found to have a T3N0M0 PDA of the pancreatic head, which was surgically resected with a classic Whipple procedure and concurrent hemicolectomy. Pathology showed pancreatic intraepithelial neoplasia grade 2 and PDA with negative surgical margins, positive perineural spread, and negative lymphovascular spread, and the patient received adjuvant chemotherapy and local radiation. In 2017, she was diagnosed with a new PDA lesion in the remaining pancreatic body far from the previous anastomosis site and was taken to surgery for a completion pancreatectomy and revision of the gastrojejunostomy. NGS was performed on both specimens. Both lesions shared identical mutations in KRAS, TP53, and CDKN2A genes. Amplifications of MYC and mutant KRAS were identified in the 2017 tumor and an ACVR1B mutation was identified in the 2011 tumor, but was not found in the 2017 tumor. Conclusions: This case demonstrates the ability to evaluate similarities between key genetic drivers from a resected primary tumor and a PDA lesion that presented in the same patient 6 years later. Histological analysis and NGS can be used to understand potential differences and similarities between lesions and may be useful in future studies as predictive markers or to provide insight into resistance mechanisms (e.g., MYC amplification).
Keywords: KRAS; MYC; Whipple procedure; metachronous; pancreatic ductal adenocarcinoma; pancreaticoduodenectomy.
Conflict of interest statement
J.R.B. is on the Scientific Advisory Board of Perthera, Inc.; M.J.P. is in an employment or leadership position with Perthera, Inc.; and C.J.Y., T.M.B., T.D., A.S., H.T., A.B.G., and S.C. have no competing financial interests.
Figures

References
-
- American Cancer Society. Cancer Facts and Figures 2013. American Cancer Society: Atlanta; 2013. Available at https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-... Accessed on May3, 2018
-
- DiMagno EP, Reber HA, Tempero MA. AGA technical review on the epidemiology, diagnosis, and treatment of pancreatic ductal adenocarcinoma. Gastroenterology. 1999;117:1464–1484 - PubMed
-
- Benassai G, Mastrorilli M, Quarto G, et al. . Factors influencing survival after resection for ductal adenocarcinoma of the head of the pancreas. J Surg Oncol. 2000;73:212–218 - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous