

The histopathological spectrum of malignant hyperthermia and rhabdomyolysis due to RYR1 mutations
- PMID: 30788618
- PMCID: PMC6420893
- DOI: 10.1007/s00415-019-09209-z
The histopathological spectrum of malignant hyperthermia and rhabdomyolysis due to RYR1 mutations
Abstract
Objective: The histopathological features of malignant hyperthermia (MH) and non-anaesthetic (mostly exertional) rhabdomyolysis (RM) due to RYR1 mutations have only been reported in a few cases.
Methods: We performed a retrospective multi-centre cohort study focussing on the histopathological features of patients with MH or RM due to RYR1 mutations (1987-2017). All muscle biopsies were reviewed by a neuromuscular pathologist. Additional morphometric and electron microscopic analysis were performed where possible.
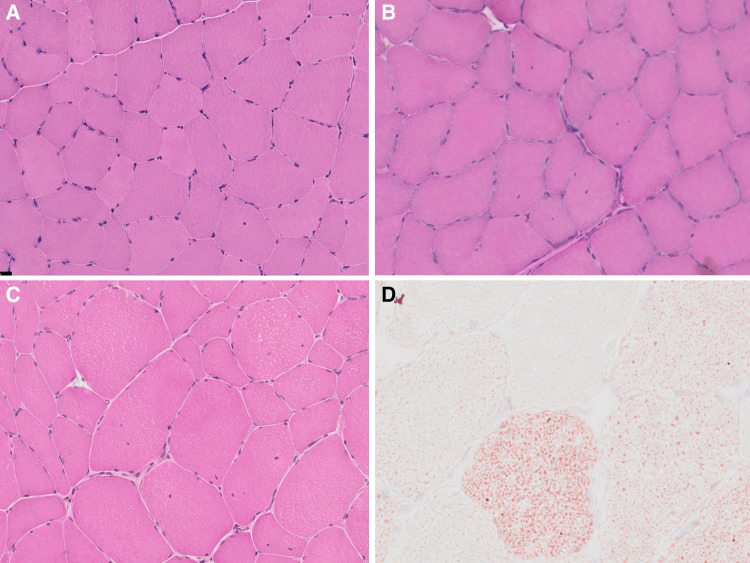
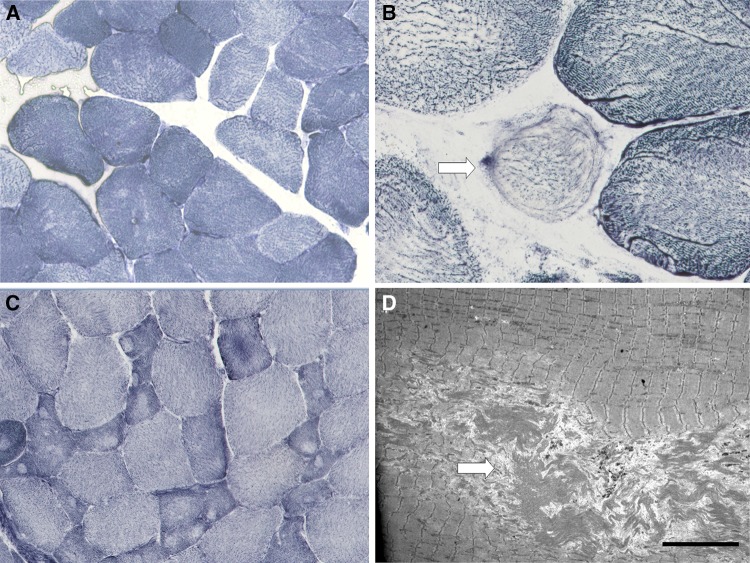
Results: Through the six participating centres we identified 50 patients from 46 families, including patients with MH (n = 31) and RM (n = 19). Overall, the biopsy of 90% of patients showed one or more myopathic features including: increased fibre size variability (n = 44), increase in the number of fibres with internal nuclei (n = 30), and type I fibre predominance (n = 13). Abnormalities on oxidative staining, generally considered to be more specifically associated with RYR1-related congenital myopathies, were observed in 52%, and included unevenness (n = 24), central cores (n = 7) and multi-minicores (n = 3). Apart from oxidative staining abnormalities more frequently observed in MH patients, the histopathological spectrum was similar between the two groups. There was no correlation between the presence of cores and the occurrence of clinically detectable weakness or presence of (likely) pathogenic variants.
Conclusions: Patients with RYR1-related MH and RM exhibit a similar histopathological spectrum, ranging from mild myopathic changes to cores and other features typical of RYR1-related congenital myopathies. Suggestive histopathological features may support RYR1 involvement, also in cases where the in vitro contracture test is not informative.
Keywords: Histology.; Malignant hyperthermia (MH); Muscle biopsy; RYR1; Rhabdomyolysis; RyR1.
Conflict of interest statement
Conflicts of interest
On behalf of all authors, the corresponding author states that there is no conflict of interest.
Ethical standards
All studies in this review have been approved by the appropriate ethics committee and have therefore been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.
Figures
References
-
- Jungbluth H, Treves S, Zorzato F, Sarkozy A, Ochala J, Sewry C et al (2018) Congenital myopathies: disorders of excitation–contraction coupling and muscle contraction. Nat Rev Neurol - PubMed
-
- Jungbluth H, Zhou H, Hartley L, Halliger-Keller B, Messina S, Longman C, et al. Minicore myopathy with ophthalmoplegia caused by mutations in the ryanodine receptor type 1 gene. Neurology. 2005;65(12):1930–1935. - PubMed
-
- Wilmshurst JM, Lillis S, Zhou H, Pillay K, Henderson H, Kress W, et al. RYR1 mutations are a common cause of congenital myopathies with central nuclei. Ann Neurol. 2010;68(5):717–726. - PubMed
-
- Clarke NF, Waddell LB, Cooper ST, Perry M, Smith RL, Kornberg AJ, et al. Recessive mutations in RYR1 are a common cause of congenital fiber type disproportion. Hum Mutat. 2010;31(7):E1544–E1550. - PubMed
-
- Dlamini N, Voermans NC, Lillis S, Stewart K, Kamsteeg EJ, Drost G, et al. Mutations in RYR1 are a common cause of exertional myalgia and rhabdomyolysis. Neuromuscul Disord. 2013;23(7):540–548. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
