

Measuring the Integration of Stereotactic Ablative Radiotherapy Plus Surgery for Early-Stage Non-Small Cell Lung Cancer: A Phase 2 Clinical Trial
- PMID: 30789648
- PMCID: PMC6512269
- DOI: 10.1001/jamaoncol.2018.6993
Measuring the Integration of Stereotactic Ablative Radiotherapy Plus Surgery for Early-Stage Non-Small Cell Lung Cancer: A Phase 2 Clinical Trial
Abstract
Importance: Stereotactic ablative radiotherapy (SABR) is a standard treatment option in patients with medically inoperable early-stage non-small cell lung cancer (NSCLC), yet the pathologic complete response (pCR) rate after SABR is unknown. Neoadjuvant SABR in patients with cancer who are fit for resection has been hypothesized to improve local control and induce antitumor immune activity, potentially leading to better outcomes.
Objectives: To determine the pCR rate after SABR and to assess oncologic and toxicity outcomes after a combined approach of neoadjuvant SABR followed by surgery.
Design, setting, and participants: A phase 2, single-arm trial, with patient accrual from September 30, 2014, to August 15, 2017 (median follow-up, 19 months), was performed at a tertiary academic cancer center. Patients 18 years or older with T1T2N0M0 NSCLC and good performance status, with adequate pulmonary reserve to undergo surgical resection, were studied.
Interventions: Patients underwent neoadjuvant SABR using a risk-adapted fractionation scheme followed by surgery 10 weeks later.
Main outcomes and measures: The pCR rate as determined by hematoxylin-eosin staining.
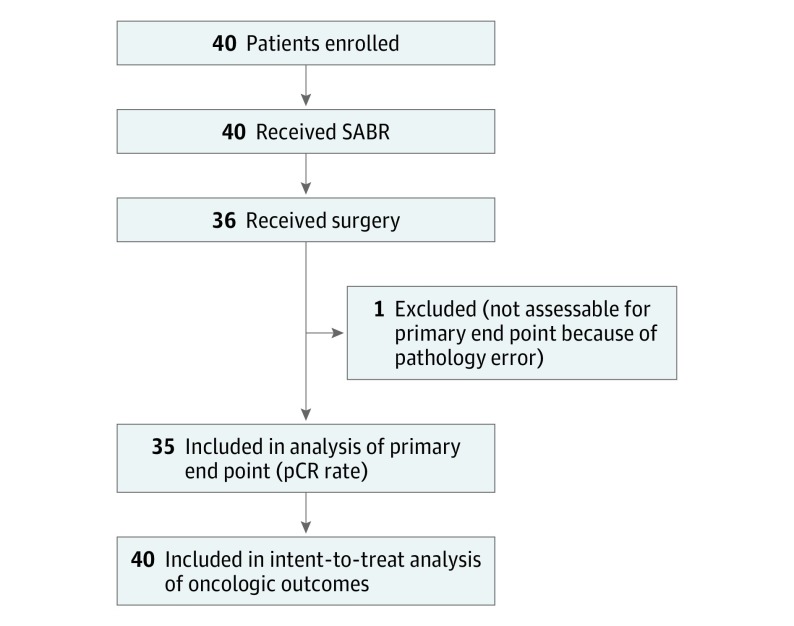
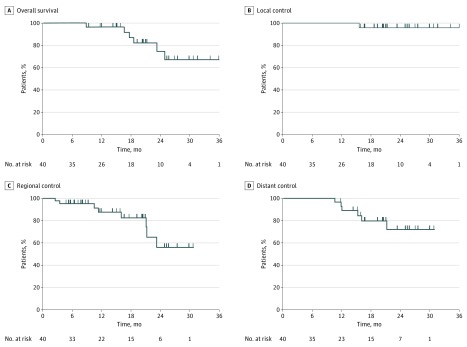
Results: Forty patients (mean [SD] age, 68 [8] years; 23 [58%] female) were enrolled. Thirty-five patients underwent surgery and were evaluable for the primary end point. The pCR rate was 60% (95% CI, 44%-76%). The 30- and 90-day postoperative mortality rates were both 0%. Grade 3 or 4 toxic effects occurred in 7 patients (18%). In patients receiving surgery, 2-year overall survival was 77% (95% CI, 48%-91%), local control was 100% (95% CI, not defined), regional control was 53% (95% CI, 22%-76%), and distant control was 76% (95% CI, 45%-91%). Quality of life did not decline after treatment, with no significant changes in mean Functional Assessment of Cancer Therapy for Lung-Trial Outcome Index score during the first year of follow-up.
Conclusions and relevance: The pCR rate after SABR for early-stage NSCLC was 60%, lower than hypothesized. The combined approach had toxic effects comparable to series of surgery alone, and there was no perioperative mortality. Further studies are needed to evaluate this combined approach compared with surgical resection alone.
Trial registration: ClinicalTrials.gov identifier: NCT02136355.
Conflict of interest statement
Figures
Comment in
-
Reproductive Viability of Cells Following Preoperative Stereotactic Ablative Radiotherapy.Int J Radiat Oncol Biol Phys. 2019 Sep 1;105(1):233-234. doi: 10.1016/j.ijrobp.2019.05.037. Int J Radiat Oncol Biol Phys. 2019. PMID: 31422814 No abstract available.
-
Stereotactic ablative radiotherapy for operable stage I non-small cell lung cancer: not ready for prime time.Ann Transl Med. 2019 Sep;7(Suppl 6):S234. doi: 10.21037/atm.2019.08.40. Ann Transl Med. 2019. PMID: 31656813 Free PMC article. No abstract available.
