

Long term outcomes and prognostics of visceral leishmaniasis in HIV infected patients with use of pentamidine as secondary prophylaxis based on CD4 level: a prospective cohort study in Ethiopia
- PMID: 30789910
- PMCID: PMC6400407
- DOI: 10.1371/journal.pntd.0007132
Long term outcomes and prognostics of visceral leishmaniasis in HIV infected patients with use of pentamidine as secondary prophylaxis based on CD4 level: a prospective cohort study in Ethiopia
Abstract
Background: The long-term treatment outcome of visceral leishmaniasis (VL) patients with HIV co-infection is complicated by a high rate of relapse, especially when the CD4 count is low. Although use of secondary prophylaxis is recommended, it is not routinely practiced and data on its effectiveness and safety are limited.
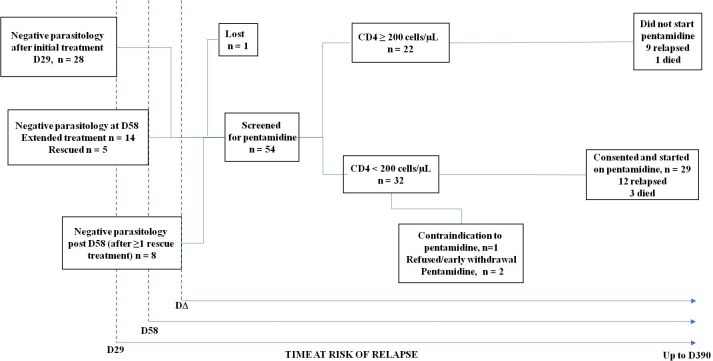
Methods: A prospective cohort study was conducted in Northwest Ethiopia from August 2014 to August 2017 (NCT02011958). HIV-VL patients were followed for up to 12 months. Patients with CD4 cell counts below 200/μL at the end of VL treatment received pentamidine prophylaxis starting one month after parasitological cure, while those with CD4 count ≥200 cells/μL were followed without secondary prophylaxis. Compliance, safety and relapse-free survival, using Kaplan-Meier analysis methods to account for variable time at risk, were summarised. Risk factors for relapse or death were analysed.
Results: Fifty-four HIV patients were followed. The probability of relapse-free survival at one year was 50% (95% confidence interval [CI]: 35-63%): 53% (30-71%) in 22 patients with CD4 ≥200 cells/μL without pentamidine prophylaxis and 46% (26-63%) in 29 with CD4 <200 cells/μL who started pentamidine. Three patients with CD4 <200 cells/μL did not start pentamidine. Amongst those with CD4 ≥200 cells/μL, VL relapse was an independent risk factor for subsequent relapse or death (adjusted rate ratio: 5.42, 95% CI: 1.1-25.8). Except for one case of renal failure which was considered possibly related to pentamidine, there were no drug-related safety concerns.
Conclusion: The relapse-free survival rate for VL patients with HIV was low. Relapse-free survival of patients with CD4 count <200cells/μL given pentamidine secondary prophylaxis appeared to be comparable to patients with a CD4 count ≥200 cells/μL not given prophylaxis. Patients with relapsed VL are at higher risk for subsequent relapse and should be considered a priority for secondary prophylaxis, irrespective of their CD4 count.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

References
-
- Diro E, Lynen L, Mohammed R, Boelaert M, Hailu A, van Griensven J (2014) High parasitological failure rate of visceral leishmaniasis to sodium stibogluconate among HIV co-infected adults in Ethiopia. PLoS Negl Trop Dis 8: e2875 10.1371/journal.pntd.0002875 PNTD-D-13-02068 [pii]. - DOI - PMC - PubMed
-
- Ritmeijer K, ter Horst R, Chane S, Aderie EM, Piening T, Collin SM, Davidson RN (2011) Limited effectiveness of high-dose liposomal amphotericin B (AmBisome) for treatment of visceral leishmaniasis in an Ethiopian population with high HIV prevalence. Clin Infect Dis 53: e152–e158. cir674 [pii] 10.1093/cid/cir674 - DOI - PubMed
-
- Dereure J, Duong TH, Lavabre-Bertrand T, Cartron G, Bastides F, Richard-Lenoble D, Dedet JP (2003) Visceral leishmaniasis. Persistence of parasites in lymph nodes after clinical cure. J Infect 47: 77–81. S0163445303000021 [pii]. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
