

Temporal Dynamics of Cerebral Blood Flow During the Acute Course of Severe Subarachnoid Hemorrhage Studied by Bedside Xenon-Enhanced CT
- PMID: 30790226
- PMCID: PMC6420446
- DOI: 10.1007/s12028-019-00675-x
Temporal Dynamics of Cerebral Blood Flow During the Acute Course of Severe Subarachnoid Hemorrhage Studied by Bedside Xenon-Enhanced CT
Abstract
Background: Compromised cerebral blood flow (CBF) is a crucial factor in delayed cerebral ischemia after subarachnoid hemorrhage (SAH). Repeated measurement of CBF may improve our understanding of the temporal dynamics following SAH. The aim of this study was to assess CBF at different phases of the acute course in poor-grade SAH patients, hypothesizing more pronounced disturbances at day 4-7, and that the initial level of CBF determines the following course of CBF.
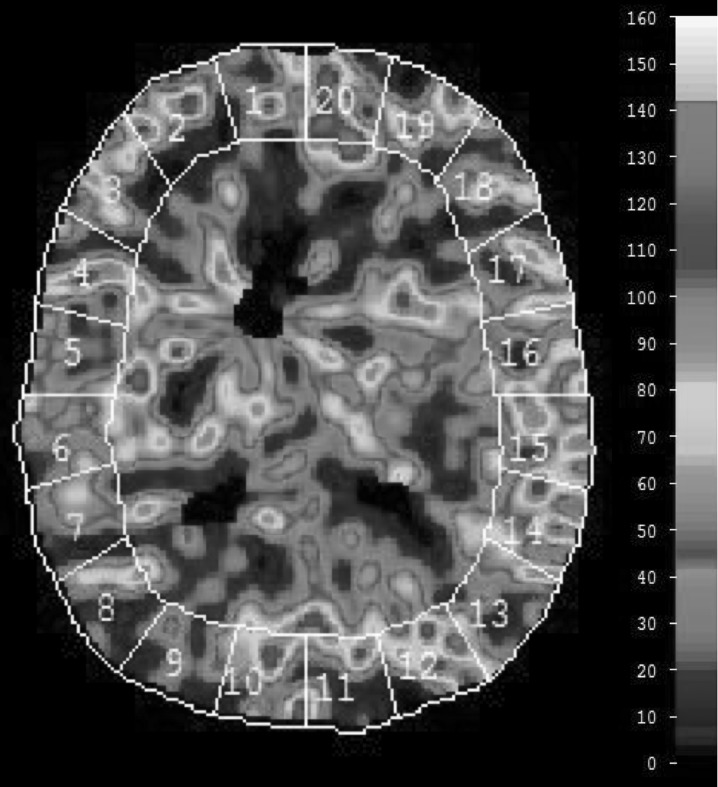
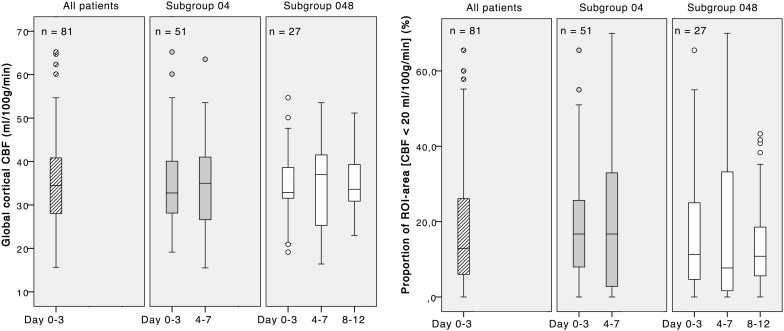
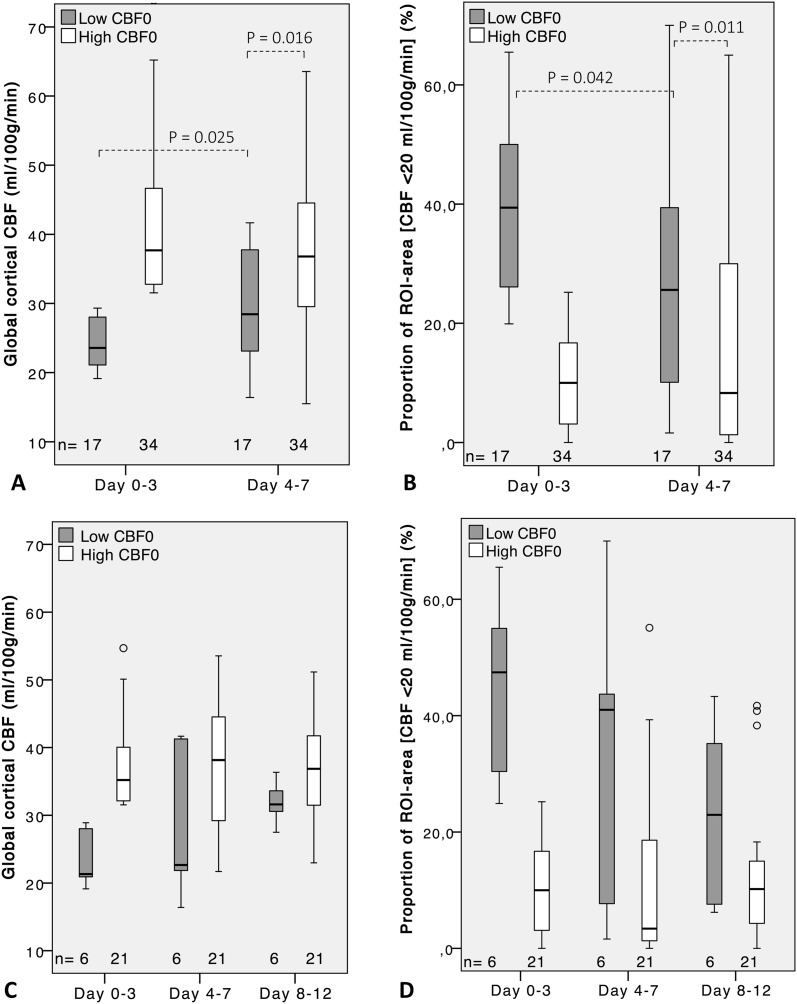
Methods: Mechanically ventilated SAH patients were scheduled for bedside measurement of regional and global cortical CBF at day 0-3, 4-7, and 8-12, using xenon-enhanced computed tomography in a mobile setup. Patients were dichotomized depending on high or low initial global cortical CBF and cutoff level 30 ml/100 g/min.
Results: Eighty-one patients were included, and 51 had measurements at day 0-3 and 4-7. In patients with high initial CBF, the level was unchanged at day 4-7; 37.7 (IQR 32.6-46.7) ml/100 g/min versus 36.8 (IQR 29.5-44.8). The low-CBF group showed a slight increase from 23.6 (IQR 21.0-28.1) ml/100 g/min to 28.4 (IQR 22.7-38.3) (P = 0.025), still markedly lower than the high-CBF group (P = 0.016). In the low-CBF group, CBF increased in patients who received hypertension, hypervolemia, and hemodilution (HHH therapy) but remained low in standard treated patients. For the subset of 27 patients examined also at day 8-12, the differences depending on initial CBF level were no longer statistically significant. Among patients with still low CBF at day 4-7, the proportion who had poor short-term outcome was 55% compared to 35% (n.s.) for patients with high CBF.
Conclusions: CBF studied in poor-grade SAH patients at large did not show any statistically significant changes over time. Stratifying patients by high or low initial CBF and whether HHH therapy was given revealed an association between low initial CBF and persistent low CBF at day 4-7. These findings may be of clinical relevance in managing SAH patients with low early CBF.
Keywords: Cerebral blood flow; Delayed cerebral ischemia; Sequential; Subarachnoid hemorrhage; Temporal; XeCT; Xenon–CT.
Conflict of interest statement
Conflicts of interest
The authors declare that they have no conflicts of interest.
Ethical Approval/Informed Consent
The study protocol was approved by the Uppsala University Regional Ethical Review Board, and informed consent was obtained from patients included or their next of kin. The study was also approved by the local Radiation Safety Authority.
Figures
Comment in
-
Commentary on "Temporal Dynamics of Cerebral Blood Flow During the Acute Course of Severe Subarachnoid Hemorrhage Studied by Bedside Xenon-Enhanced CT".Neurocrit Care. 2019 Apr;30(2):291-292. doi: 10.1007/s12028-019-00698-4. Neurocrit Care. 2019. PMID: 30815775 No abstract available.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
