

Mechanisms of Neurodegeneration and Axonal Dysfunction in Progressive Multiple Sclerosis
- PMID: 30791637
- PMCID: PMC6466454
- DOI: 10.3390/biomedicines7010014
Mechanisms of Neurodegeneration and Axonal Dysfunction in Progressive Multiple Sclerosis
Abstract
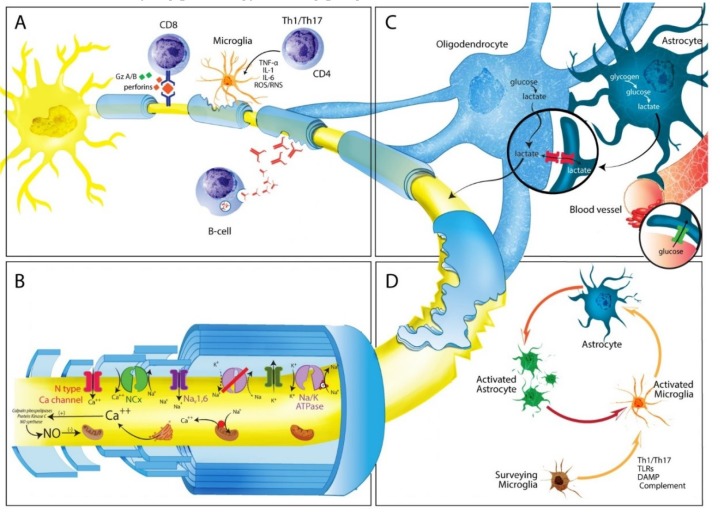
Multiple Sclerosis (MS) is a major cause of neurological disability, which increases predominantly during disease progression as a result of cortical and grey matter structures involvement. The gradual accumulation of disability characteristic of the disease seems to also result from a different set of mechanisms, including in particular immune reactions confined to the Central Nervous System such as: (a) B-cell dysregulation, (b) CD8⁺ T cells causing demyelination or axonal/neuronal damage, and (c) microglial cell activation associated with neuritic transection found in cortical demyelinating lesions. Other potential drivers of neurodegeneration are generation of oxygen and nitrogen reactive species, and mitochondrial damage, inducing impaired energy production, and intra-axonal accumulation of Ca2+, which in turn activates a variety of catabolic enzymes ultimately leading to progressive proteolytic degradation of cytoskeleton proteins. Loss of axon energy provided by oligodendrocytes determines further axonal degeneration and neuronal loss. Clearly, these different mechanisms are not mutually exclusive and could act in combination. Given the multifactorial pathophysiology of progressive MS, many potential therapeutic targets could be investigated in the future. This remains however, an objective that has yet to be undertaken.
Keywords: autoimmunity; axon; cortex; demyelination; mitochondria; multiple sclerosis; myelin; neurodegeneration; oligodendrocyte; progressive multiple sclerosis.
Conflict of interest statement
J.C. is a board member of Merck-Serono Argentina, Biogen-Idec LATAM, Merck-Serono LATAM, and Genzyme global. Jorge Correale has received reimbursement for developing educational presentations for Merck-Serono Argentina, Merck-Serono LATAM, Biogen-Idec Argentina, Genzyme Argentina, and TEVA Argentina as well as professional travel/accommodations stipends. M.M. has nothing to disclose. M.C.Y. has received reimbursement for developing educational presentations and for travel/accommodations stipends from Merck-Serono Argentina, Biogen-Idec Argentina, Genzyme Argentina, Bayer Inc, Novartis Argentina and TEVA-Tuteur Argentina.
Figures
References
-
- Skulina C., Schmidt S., Dornmair K., Babbe H., Roers A., Rajewsky K., Wekerle H., Hohlfeld R., Goebels N. Multiple sclerosis: Brain-infiltrating CD8+ T cells persist as clonal expansions in the cerebrospinal fluid and blood. Proc. Natl. Acad. Sci. USA. 2004;101:2428–2433. doi: 10.1073/pnas.0308689100. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
