

Not only Alagille syndrome. Syndromic paucity of interlobular bile ducts secondary to HNF1β deficiency: a case report and literature review
- PMID: 30791938
- PMCID: PMC6385394
- DOI: 10.1186/s13052-019-0617-y
Not only Alagille syndrome. Syndromic paucity of interlobular bile ducts secondary to HNF1β deficiency: a case report and literature review
Abstract
Background: paucity of interlobular bile ducts is an important observation at liver biopsy in the diagnostic work-up of neonatal cholestasis. To date, other than in the Alagille syndrome, syndromic paucity of interlobular bile ducts has been documented in four cholestatic neonates with HFN1β mutations. A syndromic phenotype, known as renal cysts and diabetes syndrome (RCAD), has been identified. This is usually characterized by a wide clinical spectrum, including renal cysts, maturity-onset diabetes of the young, exocrine pancreatic insufficiency, urogenital abnormalities and a not well established liver involvement. Herein we report a novel case of paucity of interlobular bile ducts due to an HFN1β defect.
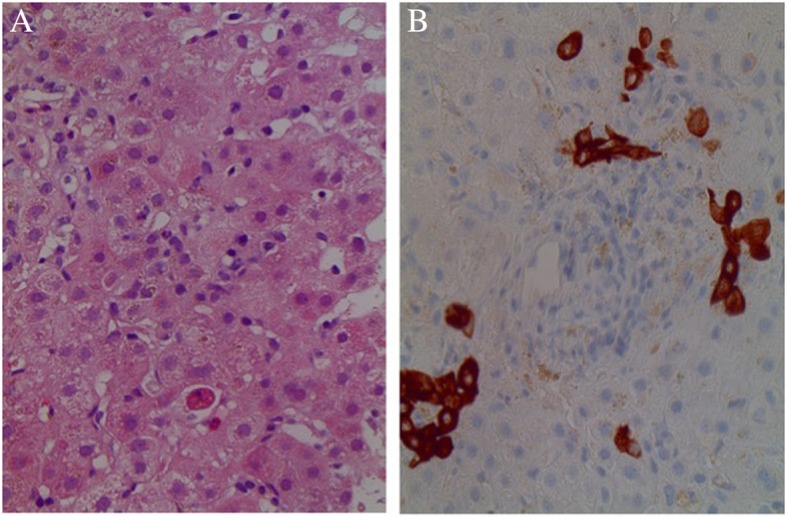
Case presentation: A 5-week-old boy was admitted to our department for cholestatic jaundice with increased gamma-glutamyl transpeptidase and an unremarkable clinical examination. He had been delivered by Caesarian section at 38 weeks' gestation from unrelated parents, with a birth weight of 2600 g (3rd percentile). Screening for cholestatic diseases, including Alagille syndrome, was negative except for a minor pulmonary artery stenosis at echocardiography and a doubt of a thoracic butterfly hemivertebra. The finding of hyperechogenic kidneys with multiple bilateral cortical cysts at ultrasound examination, associated with moderately impaired renal function with proteinuria, polyuria and metabolic acidosis, was suggestive of ciliopathy. A liver biopsy was performed revealing paucity of interlobular bile ducts, thus the diagnosis of Alagille syndrome was reconsidered. Although genetic tests for liver cholestatic diseases were performed with negative results for Alagille syndrome (JAG1 and NOTCH2), a de-novo missense mutation of HNF1β gene was detected. At 18 months of age our patient has persistent cholestasis and his itching is not under satisfactory control.
Conclusions: Alagille syndrome may not be the only syndrome determining paucity of interlobular bile ducts in neonates presenting with cholestasis and renal impairment, especially in small for gestational age newborns. We suggest that HNF1β deficiency should also be ruled out, taking into consideration HNF1β mutations, together with Alagille syndrome, in next generation sequencing strategies in neonates with cholestasis, renal impairment and/or paucity of interlobular bile ducts at liver biopsy.
Keywords: Alagille syndrome; Ciliopathy; HNF1β mutations; Paucity of interlobular bile ducts; Renal cysts.
Conflict of interest statement
Ethics approval and consent to participate
parental informed consent for publication was obtained.
Consent for publication
written informed consent was obtained from the patient’s legal guardians for publication of this case report and any accompanying images.
Competing interests
the authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
