

Comparing clinical judgment with the MySurgeryRisk algorithm for preoperative risk assessment: A pilot usability study
- PMID: 30792011
- PMCID: PMC6502657
- DOI: 10.1016/j.surg.2019.01.002
Comparing clinical judgment with the MySurgeryRisk algorithm for preoperative risk assessment: A pilot usability study
Abstract
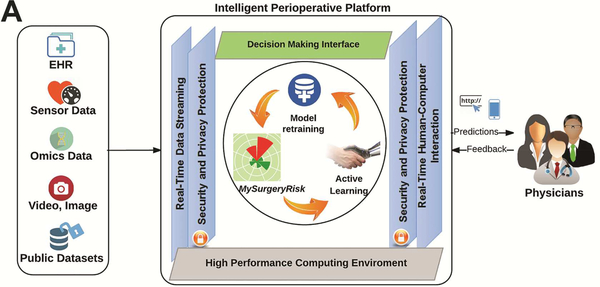
Background: Major postoperative complications are associated with increased cost and mortality. The complexity of electronic health records overwhelms physicians' abilities to use the information for optimal and timely preoperative risk assessment. We hypothesized that data-driven, predictive-risk algorithms implemented in an intelligent decision-support platform simplify and augment physicians' risk assessments.
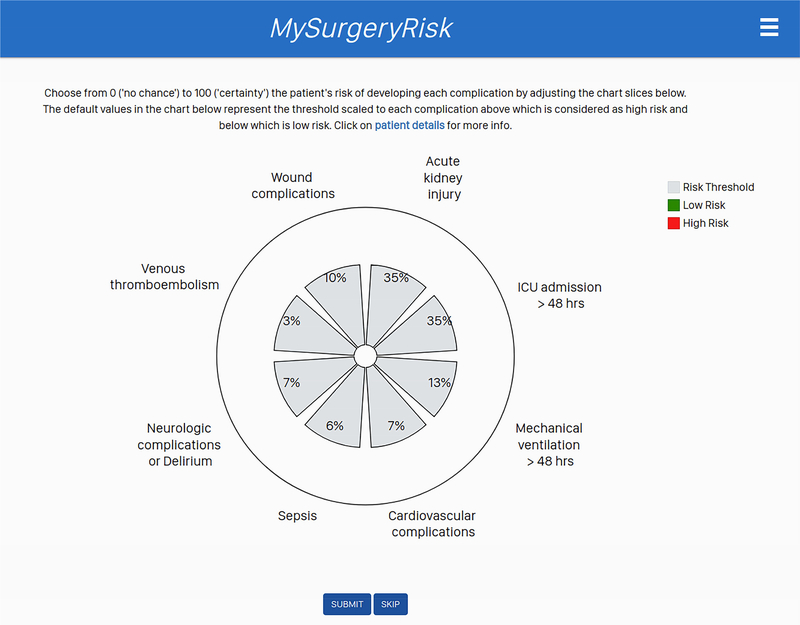
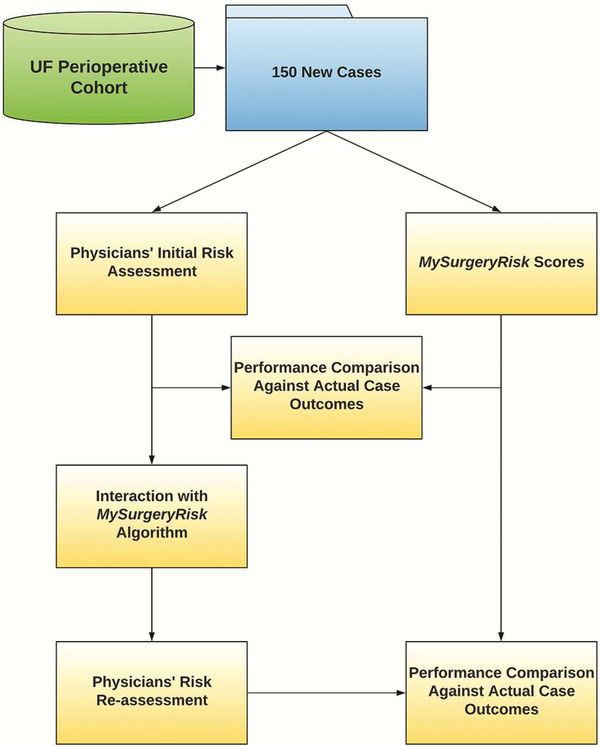
Methods: This prospective, nonrandomized pilot study of 20 physicians at a quaternary academic medical center compared the usability and accuracy of preoperative risk assessment between physicians and MySurgeryRisk, a validated, machine-learning algorithm, using a simulated workflow for the real-time, intelligent decision-support platform. We used area under the receiver operating characteristic curve to compare the accuracy of physicians' risk assessment for six postoperative complications before and after interaction with the algorithm for 150 clinical cases.
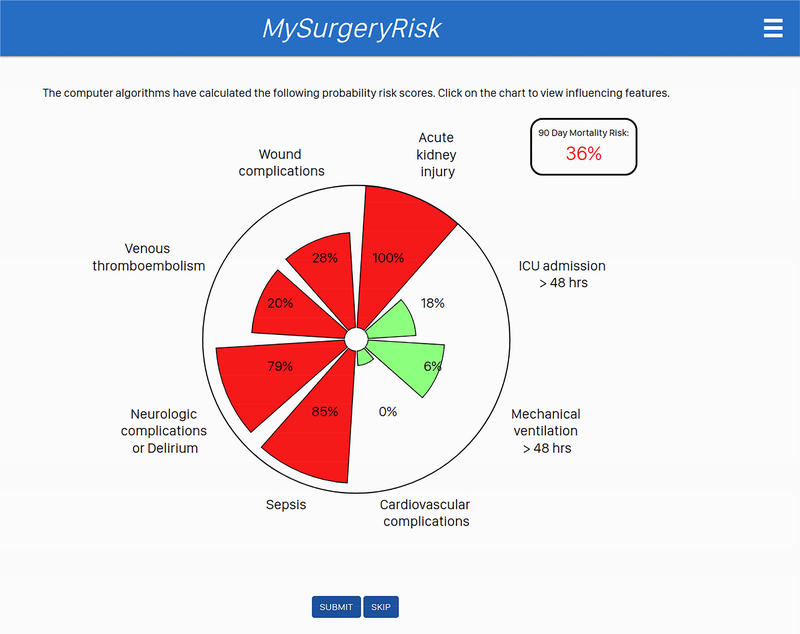
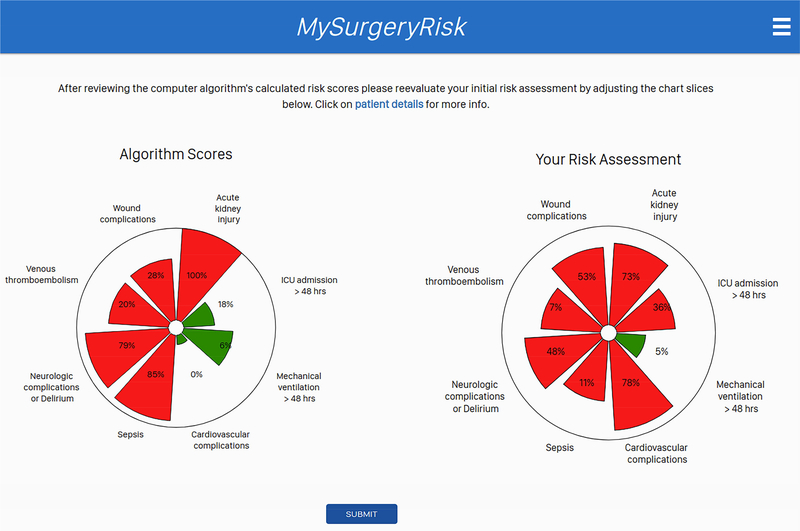
Results: The area under the receiver operating characteristic curve of the MySurgeryRisk algorithm ranged between 0.73 and 0.85 and was significantly better than physicians' initial risk assessments (area under the receiver operating characteristic curve between 0.47 and 0.69) for all postoperative complications except cardiovascular. After interaction with the algorithm, the physicians significantly improved their risk assessment for acute kidney injury and for an intensive care unit admission greater than 48 hours, resulting in a net improvement of reclassification of 12% and 16%, respectively. Physicians rated the algorithm as easy to use and useful.
Conclusion: Implementation of a validated, MySurgeryRisk computational algorithm for real-time predictive analytics with data derived from the electronic health records to augment physicians' decision-making is feasible and accepted by physicians. Early involvement of physicians as key stakeholders in both design and implementation of this technology will be crucial for its future success.
Copyright © 2019 Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
References
-
- Tepas JJ, Rimar JM, Hsiao AL, Nussbaum MS. Automated analysis of electronic medical record data reflects the pathophysiology of operative complications. Surgery. 2013;154:918–24. - PubMed
-
- Lagu T, Rothberg MB, Shieh MS, Pekow PS, Steingrub JS, Lindenauer PK. Hospitalizations, costs, and outcomes of severe sepsis in the United States 2003 to 2007. Crit Care Med. 2012;40:754–61. - PubMed
-
- Silber JH, Rosenbaum PR, Trudeau ME, Chen W, Zhang X, Kelz RR, et al. Changes in prognosis after the first postoperative complication. Med Care. 2005;43:122–31. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
