

Wisdom of the caregivers: pooling individual subjective reports to diagnose states of consciousness in brain-injured patients, a monocentric prospective study
- PMID: 30792234
- PMCID: PMC6410088
- DOI: 10.1136/bmjopen-2018-026211
Wisdom of the caregivers: pooling individual subjective reports to diagnose states of consciousness in brain-injured patients, a monocentric prospective study
Abstract
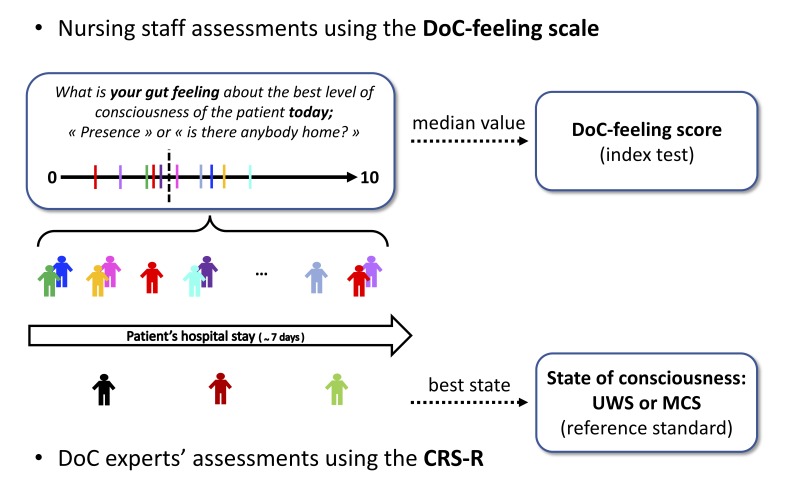
Objectives: The clinical distinction between vegetative state/unresponsive wakefulness syndrome (UWS) and minimally conscious state (MCS) is a key step to elaborate a prognosis and formulate an appropriate medical plan for any patient suffering from disorders of consciousness (DoC). However, this assessment is often challenging and may require specialised expertise. In this study, we hypothesised that pooling subjective reports of the level of consciousness of a given patient across several nursing staff members can be used to clinically detect MCS.
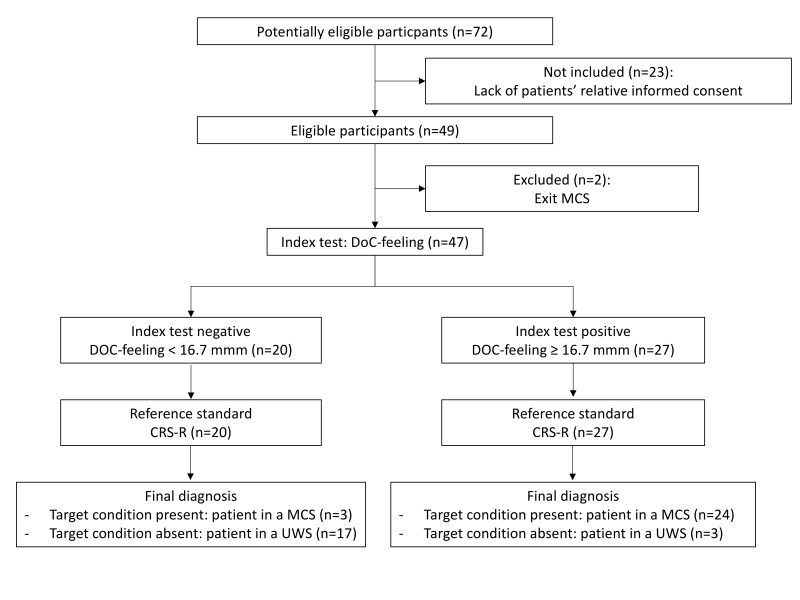
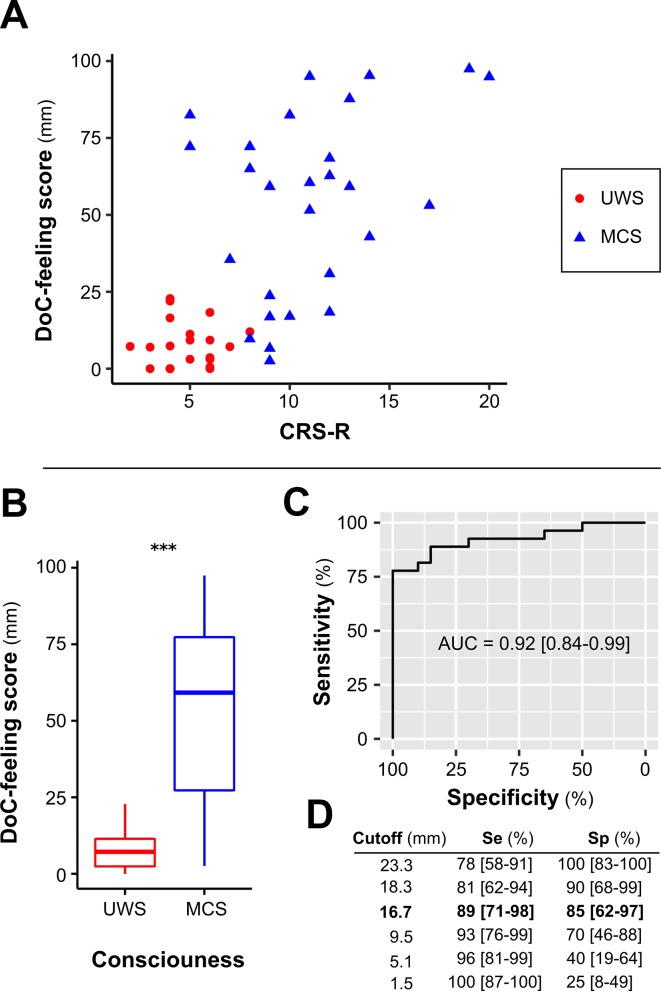
Setting and participants: Patients referred to consciousness assessment were prospectively screened. MCS (target condition) was defined according to the best Coma Recovery Scale-Revised score (CRS-R) obtained from expert physicians (reference standard). 'DoC-feeling' score was defined as the median of individual subjective reports pooled from multiple staff members during a week of hospitalisation (index test). Individual ratings were collected at the end of each shift using a 100 mm Visual Analogue Scale, blinded from the reference standard. Diagnostic accuracy was evaluated using area under the receiver operating characteristic curve (AUC), sensitivity and specificity metrics.
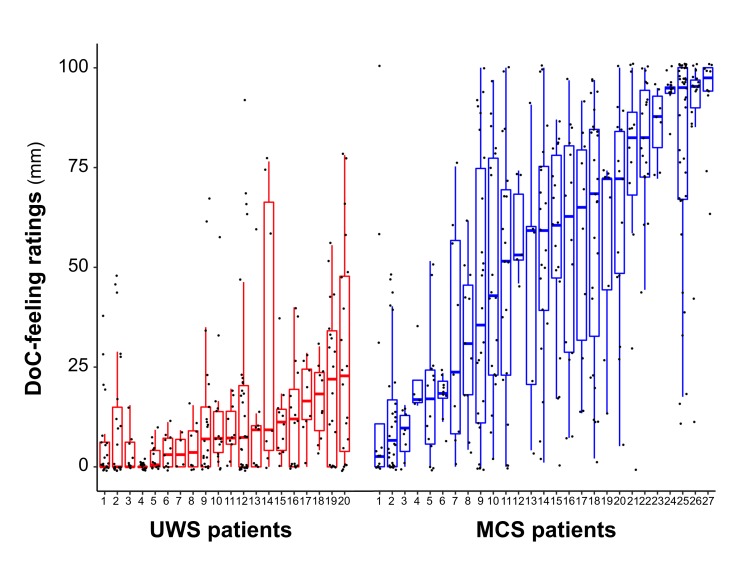
Results: 692 ratings performed by 83 nursing staff members were collected from 47 patients. Twenty patients were diagnosed with UWS and 27 with MCS. DoC-feeling scores obtained by pooling all individual ratings obtained for a given patient were significantly greater in patients with MCS than with UWS (59.2 mm (IQR: 27.3-77.3) vs 7.2 mm (IQR: 2.4-11.4); p<0.001) yielding an AUC of 0.92 (95% CI 0.84 to 0.99).
Conclusions: DoC-feeling capitalises on the expertise of nursing staff to evaluate patients' consciousness. Together with the CRS-R as well as with brain imaging, DoC-feeling might improve diagnostic and prognostic accuracy of patients with DoC.
Keywords: clinical assessment; coma recovery scale - revised; diagnosis; disorders of consciousness; group decision making; minimally conscious state.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical