

Intensified therapies improve survival and identification of novel prognostic factors for placental-site and epithelioid trophoblastic tumours
- PMID: 30792530
- PMCID: PMC6461960
- DOI: 10.1038/s41416-019-0402-0
Intensified therapies improve survival and identification of novel prognostic factors for placental-site and epithelioid trophoblastic tumours
Abstract
Background: Placental-site trophoblastic (PSTT) and epithelioid trophoblastic tumours (ETT) are the rarest malignant forms of gestational trophoblastic disease (GTD). Our prior work demonstrated that an interval of ≥48 months from the antecedent pregnancy was associated with 100% death rate, independent of the stage. Here, we assess whether modified treatments for these patients have increased survival and identify new prognostic factors.
Methods: The United Kingdom GTD database was screened to identify all PSTT/ETT cases diagnosed between 1973 and 2014. Data and survival outcomes from our prior patient cohort (1976-2006) were compared to our new modern cohort (2007-2014), when intensified treatments were introduced.
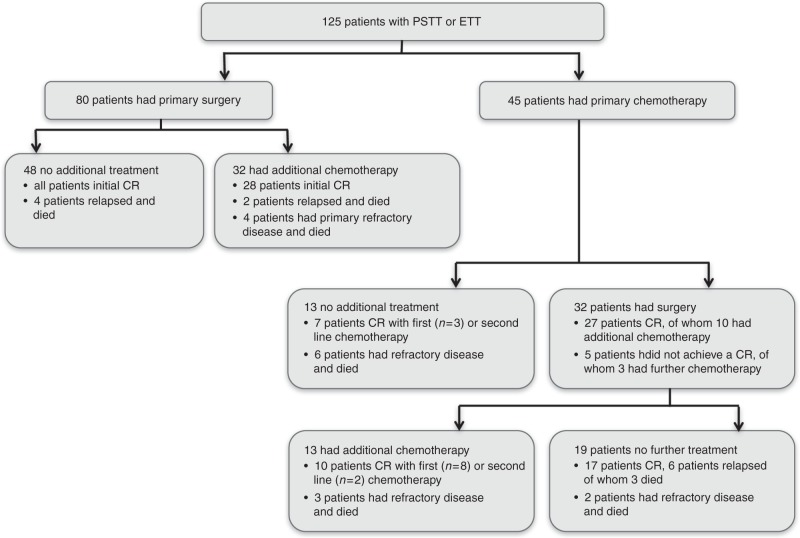
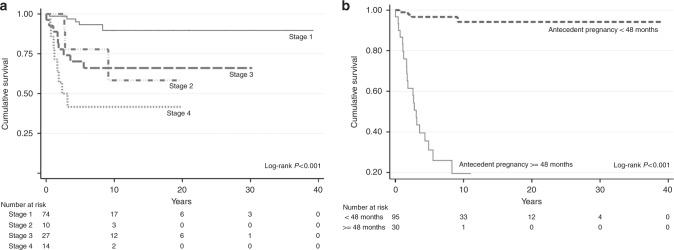
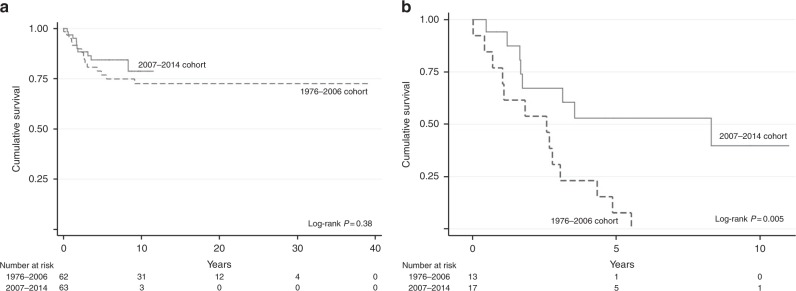
Results: Of 54,743 GTD patients, 125 (0.23%) were diagnosed with PSTT and/or ETT. Probability of survival at 5 and 10 years following treatment was 80% (95% CI 72.8-87.6%) and 75% (95% CI 66.3-84.3%), respectively. Univariate analysis identified five prognostic factors for reduced overall survival (age, FIGO stage, time since antecedent pregnancy, hCG level, mitotic index) of which stage IV disease (HR 6.18, 95% CI 1.61-23.81, p = 0.008) and interval ≥48 months since antecedent pregnancy (HR 14.57, 95% CI 4.17-50.96, p < 0.001) were most significant on multivariable analysis. No significant differences in prognostic factors were seen between the old and new patient cohort. However, the new cohort received significantly more cisplatin-based and high-dose chemotherapy, and patients with an interval ≥48 months demonstrated an improved median overall survival (8.3 years, 95% CI 1.53-15.1, versus 2.6 years, 95% CI 0.73-4.44, p = 0.·005).
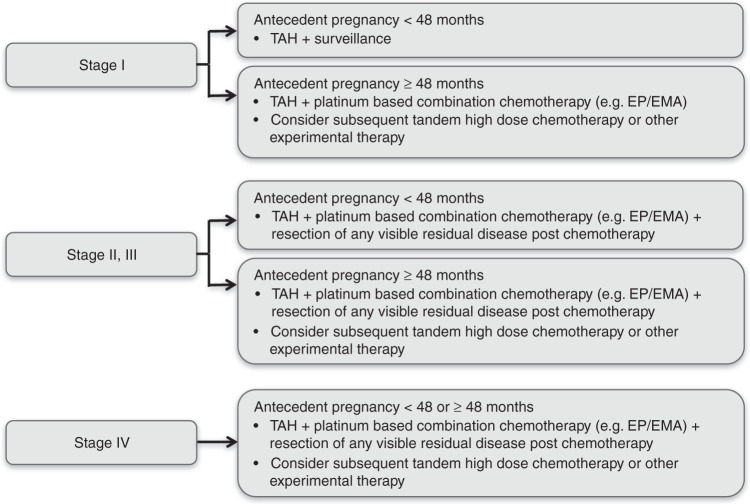
Conclusion: PSTT/ETT with advanced FIGO stage or an interval ≥48 months from their last known pregnancy have poorer outcomes. Platinum-based and high-dose chemotherapy may help to improve survival in poor-prognosis patients.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Seckl MJ, et al. Gestational trophoblastic disease: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2013;24(Suppl. 6):vi39–vi50. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
