

Analysis of a new best-practice advisory on time to initiation of antibiotics in surgical intensive care unit patients with septic shock
- PMID: 30792760
- PMCID: PMC6376576
- DOI: 10.1177/1751143718767059
Analysis of a new best-practice advisory on time to initiation of antibiotics in surgical intensive care unit patients with septic shock
Abstract
Background: Early administration of antibiotics in septic shock is associated with decreased mortality. Promptly identifying sepsis and eliciting a response are necessary to reduce time to antibiotic administration.
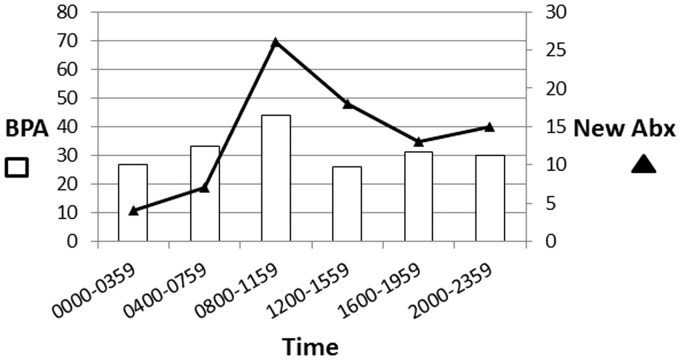
Methods: A best-practice advisory was introduced in the surgical intensive care unit to identify patients with septic shock and promote timely action. The best-practice advisory is triggered by blood culture orders and vasopressor administration within 24 h. The nurse or provider who triggers the alert may send an automatic notification to the intensive care unit resident, clinical pharmacist, and charge nurse, prompting bedside response and closer evaluation. Patients who met best-practice advisory criteria in the surgical intensive care unit from May 2016 through March 2017 were included. Outcomes included changes in antibiotics within 24 h, response to best-practice advisory, and time-to-antibiotics. Time-to-antibiotics was compared between a retrospective pre-intervention period and a six-month prospective post-intervention period defined by launch of the new best-practice advisory in September 2016. Data were analyzed by chi square, Mann-Whitney U, and Kruskal-Wallis.
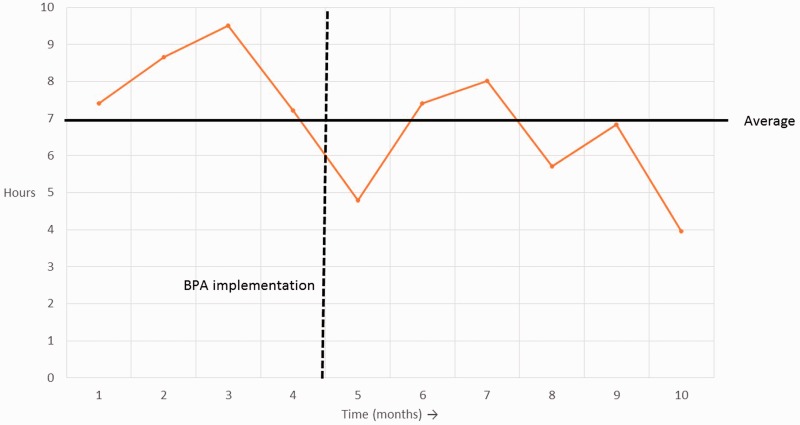
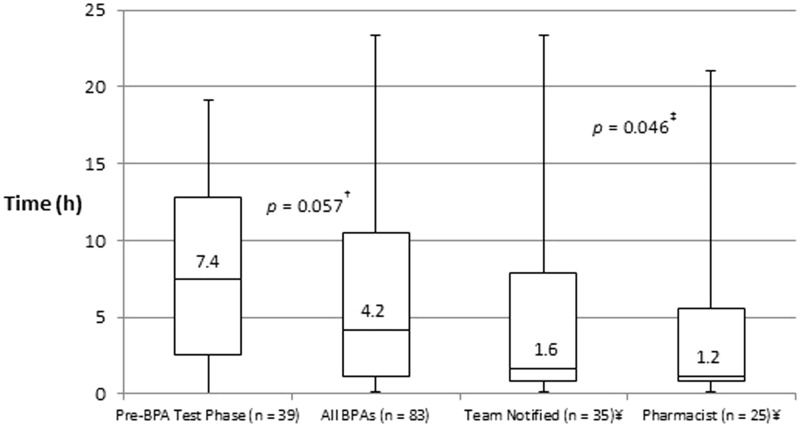
Results: During the first six months of best-practice advisory implementation, 191 alerts were triggered by 97 unique patients. Alert notification was transmitted in 79 best-practice advisories (41%), with pharmacist bedside response in 53 (67%). New antibiotics were started within 24 h following 83 best-practice advisories (43%). There was a trend toward decreased time-to-antibiotics following implementation of the best-practice advisory (7.4 vs. 4.2 h, p = 0.057). Compared to the entire cohort, time-to-antibiotics was shorter when the team was notified and when a pharmacist responded to the bedside (4.2 vs. 1.6 vs. 1.2 hours).
Conclusions: A new best-practice advisory has been effective at eliciting a rapid response and reducing the time-to-antibiotics in surgical intensive care unit patients with septic shock. Team notification and pharmacist response are associated with decreased time-to-antibiotics.
Keywords: Sepsis; antibiotics; electronic alert; intensive care unit; septic shock.
Figures
References
-
- Kumar A, Roberts D, Wood KE, et al. Duration of hypotention before initiation of effective antimicrobial therapy is the critical determinant of survival in human septic shock. Crit Care Med 2006; 34: 1589–1596. - PubMed
-
- Ferrer R, Martin-Loeches I, Philips G, et al. Empiric antibiotic treatment reduces mortality in severe sepsis and septic shock from the first hour: results from a guideline-based performance improvement program. Crit Care Med 2014; 42: 1749–1755. - PubMed
-
- Gaieski DF, Edwards JM, Kallan MJ, et al. Benchmarking the incidence and mortality of severe sepsis in the United States. Crit Care Med 2013; 41: 1167–1174. - PubMed
-
- Rhodes A, Evans LE, Alhazzani W, et al. Surviving sepsis campaign: international guidelines for management of severe sepsis and septic shock: 2016. Crit Care Med 2017; 45: 486–552. - PubMed
-
- Dellinger RP, Levy MM, Rhodes A, et al. Surviving Sepsis Campaign Guidelines Committee including the Pediatric Subgroup. Surviving sepsis campaign: international guidelines for management of severe sepsis and septic shock: 2012. Crit Care Med 2013; 41: 580–637. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous