

Detection of Circulating Tumor DNA in Patients With Leiomyosarcoma With Progressive Disease
- PMID: 30793095
- PMCID: PMC6380497
- DOI: 10.1200/PO.18.00235
Detection of Circulating Tumor DNA in Patients With Leiomyosarcoma With Progressive Disease
Abstract
Purpose: Leiomyosarcoma (LMS) is a soft tissue sarcoma characterized by multiple copy number alterations (CNAs) and without common recurrent single nucleotide variants. We evaluated the feasibility of detecting circulating tumor DNA (ctDNA) with next-generation sequencing in a cohort of patients with LMS whose tumor burden ranged from no evidence of disease to metastatic progressive disease.
Patients and methods: Cell-free DNA in plasma samples and paired genomic DNA from resected tumors were evaluated from patients with LMS by ultra-low passage whole genome sequencing (ULP-WGS). Sequencing reads were aligned to the human genome and CNAs identified in cell-free DNA and tumor DNA by ichorCNA software to determine the presence of ctDNA. Clinical data were reviewed to assess disease burden and clinicopathologic features.
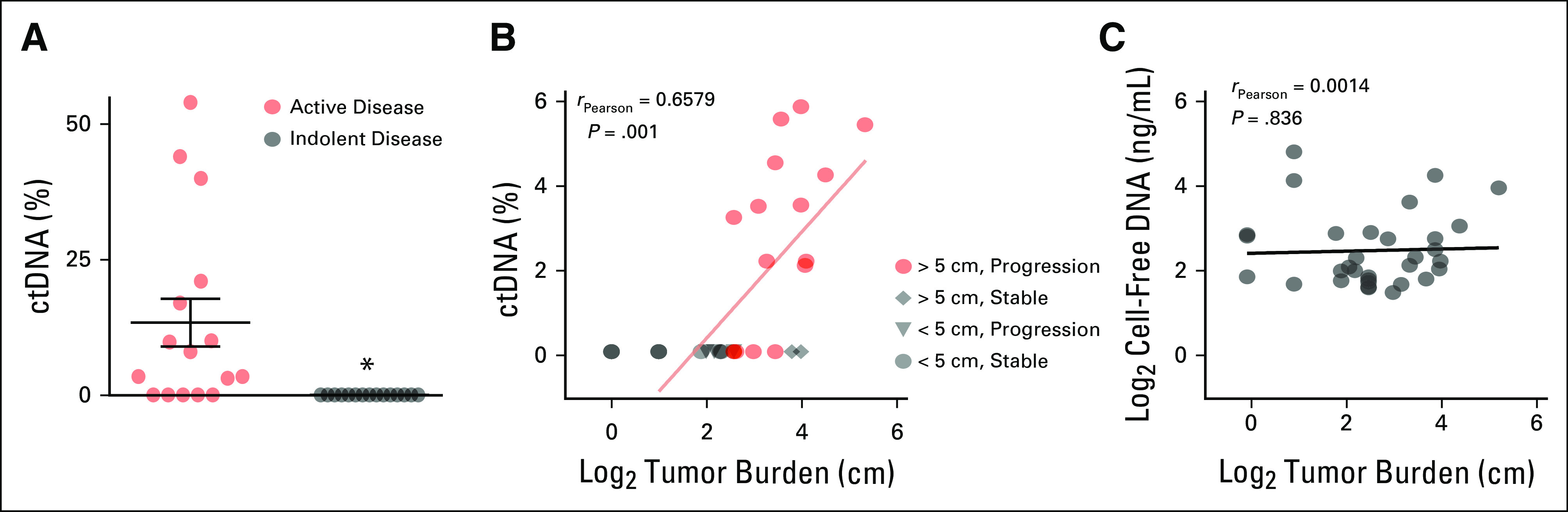
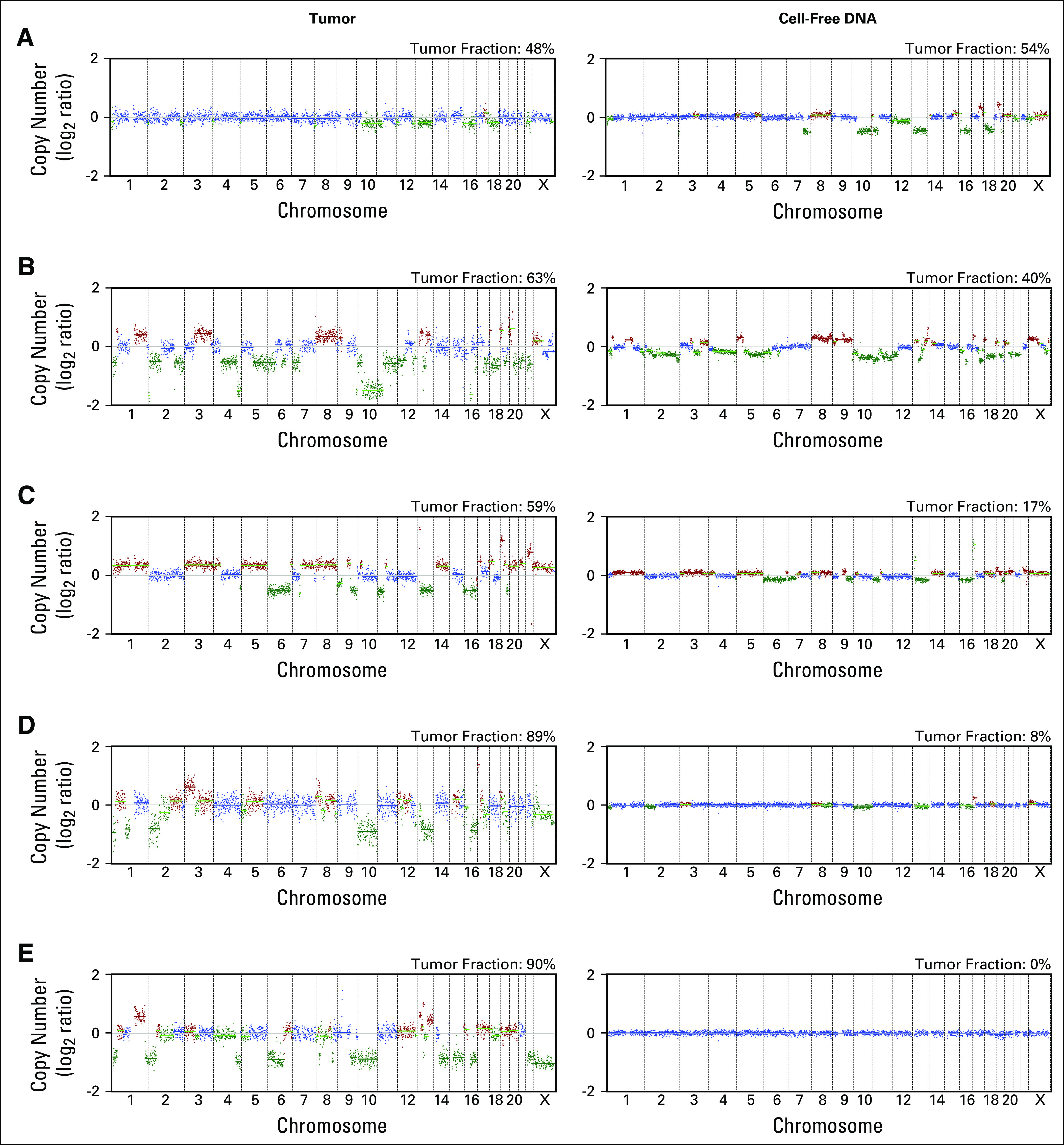
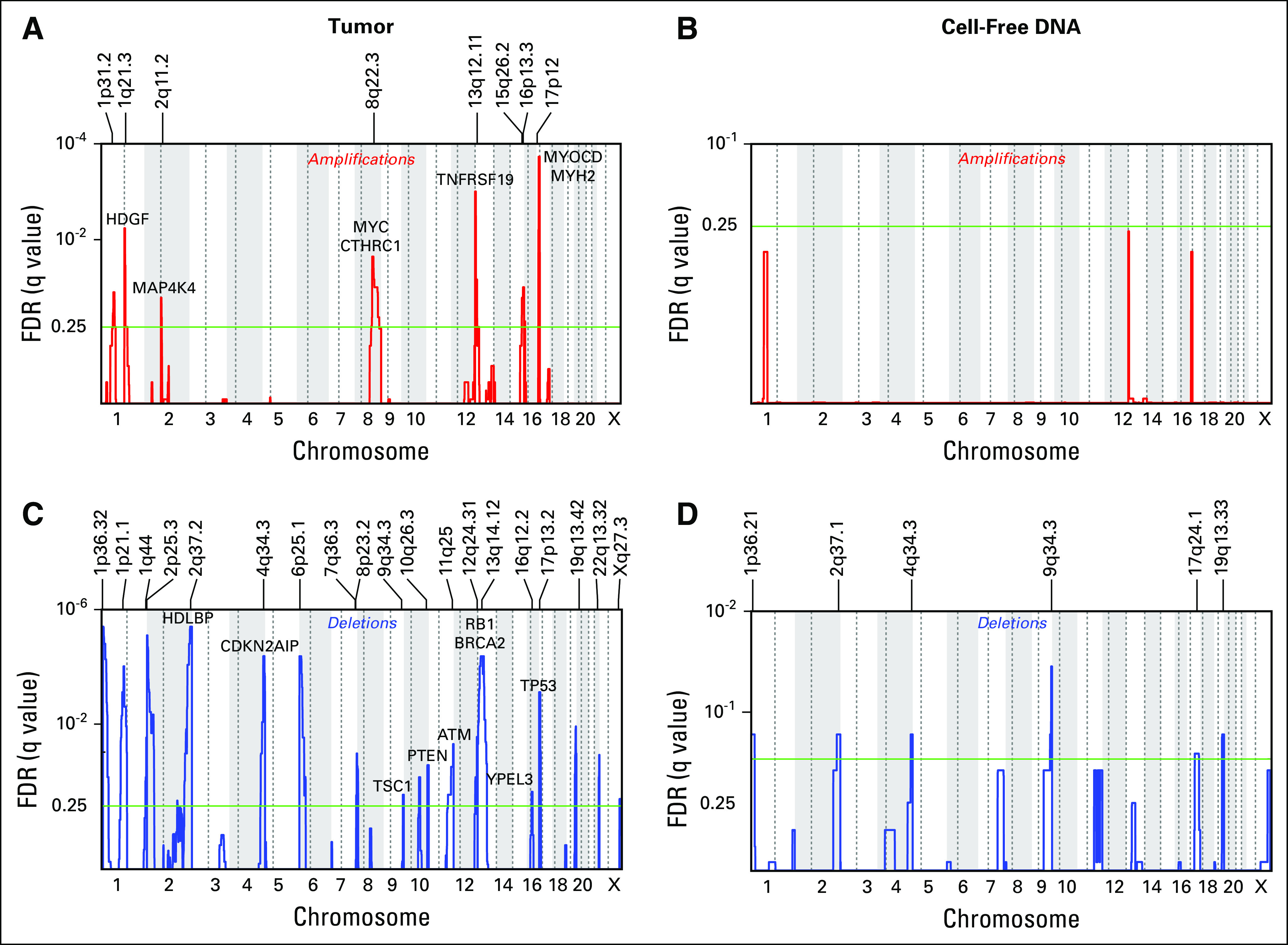
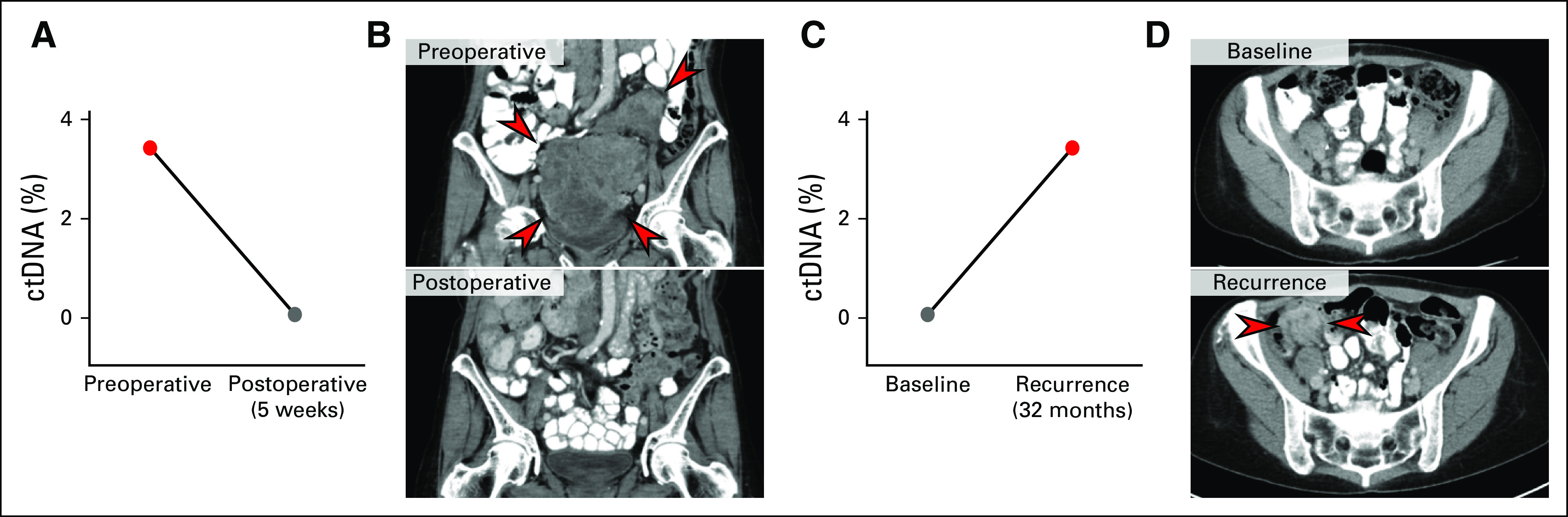
Results: We identified LMS ctDNA in eleven of sixteen patients (69%) with disease progression and total tumor burden over 5 cm. Sixteen patients with stable disease or low disease burden at the time of blood draw were found to have no detectable ctDNA. Higher ctDNA fraction of total cell-free DNA was associated with increasing tumor size and disease progression. Conserved CNAs were found between primary tumors and ctDNA in each case, and recurrent CNAs were found across LMS samples. ctDNA levels declined following resection of progressive disease in one case and became detectable upon disease relapse in another individual patient.
Conclusion: These results suggest that ctDNA, assayed by a widely available sequencing approach, may be useful as a biomarker for a subset of uterine and extrauterine LMS. Higher levels of ctDNA correlate with tumor size and disease progression. Liquid biopsies may assist in guiding treatment decisions, monitoring response to systemic therapy, surveying for disease recurrence and differentiating benign and malignant smooth muscle tumors.
Keywords: Leiomyosarcoma; circulating tumor DNA; copy number alteration; liquid biopsy.
Conflict of interest statement
AUTHORS’ DISCLOSURES OF POTENTIAL CONFLICTS OF INTEREST Matthew L. Hemming No relationship to disclose Kelly S. Klega No relationship to disclose Justin Rhoades No relationship to disclose Gavin Ha Patent application: WO2017161175A1 Kate E. Acker No relationship to disclose Jessica L. Andersen No relationship to disclose Anwesha Nag No relationship to disclose Aaron R. Thorner No relationship to disclose Chandrajit P. Raut No relationship to disclose Suzanne George Consulting or Advisory Role: Blueprint Medicines, Deciphera Pharmaceuticals Research Funding: Bayer, Pfizer, Novartis Brian D. Crompton No relationship to disclose
Figures
References
-
- Toro JR, Travis LB, Wu HJ, et al. Incidence patterns of soft tissue sarcomas, regardless of primary site, in the Surveillance, Epidemiology and End Results program, 1978-2001: An analysis of 26,758 cases. Int J Cancer. 2006;119:2922–2930. - PubMed
-
- Bjerkehagen B, Smeland S, Walberg L, et al. Radiation-induced sarcoma: 25-year experience from the Norwegian Radium Hospital. Acta Oncol. 2008;47:1475–1482. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
