

Development of an integrated multimodal optical imaging system with real-time image analysis for the evaluation of oral premalignant lesions
- PMID: 30793567
- PMCID: PMC6383051
- DOI: 10.1117/1.JBO.24.2.025003
Development of an integrated multimodal optical imaging system with real-time image analysis for the evaluation of oral premalignant lesions
Abstract
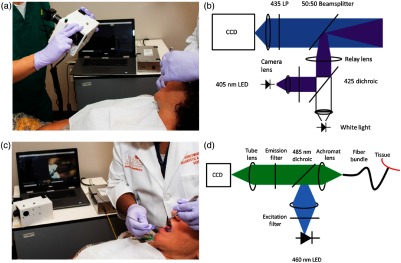
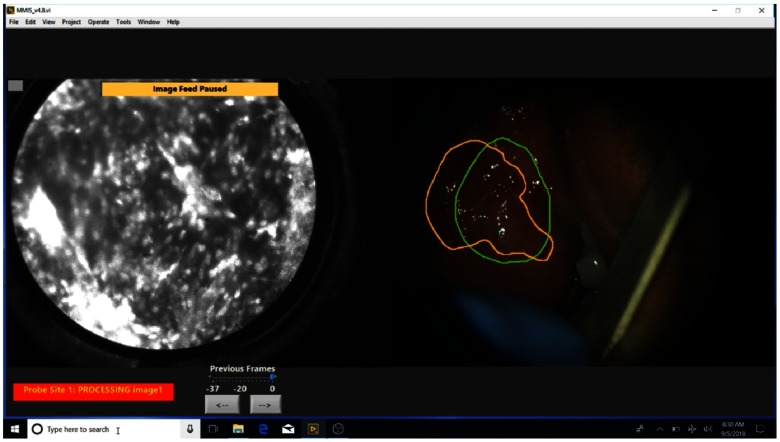
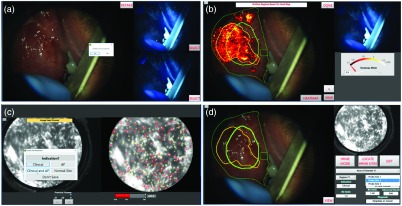
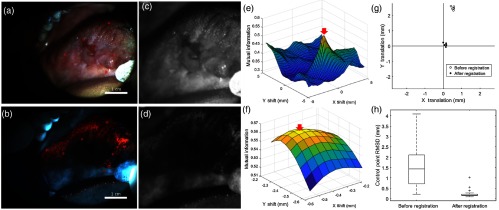
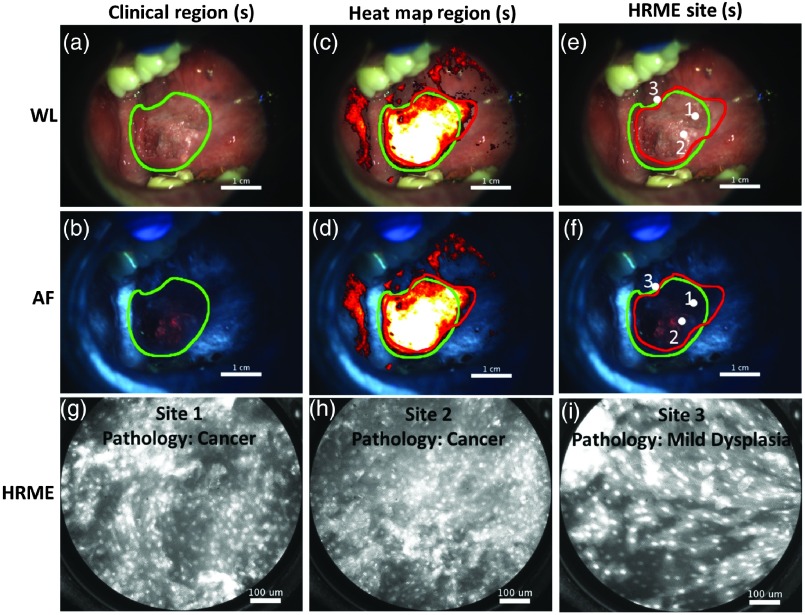
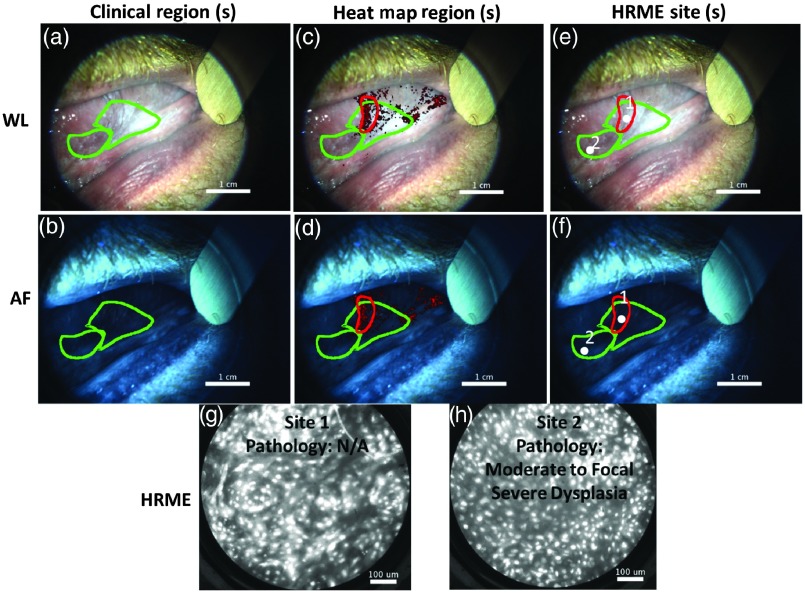
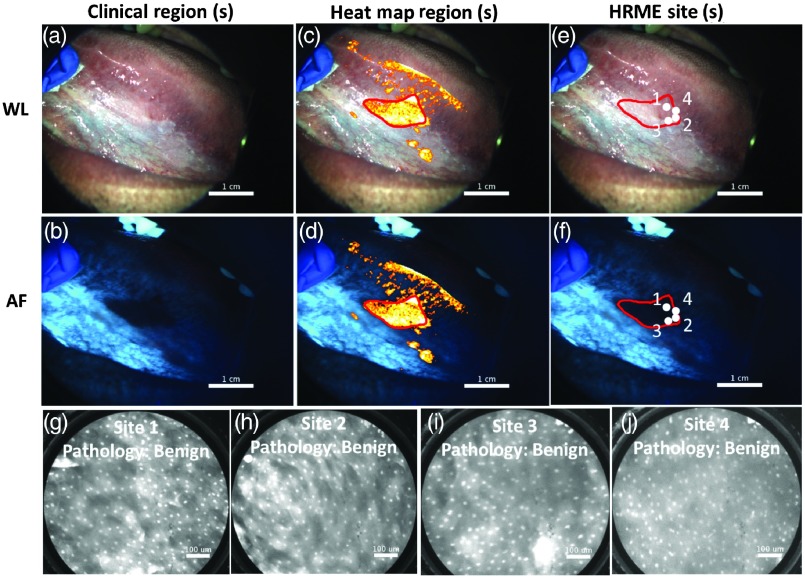
Oral premalignant lesions (OPLs), such as leukoplakia, are at risk of malignant transformation to oral cancer. Clinicians can elect to biopsy OPLs and assess them for dysplasia, a marker of increased risk. However, it is challenging to decide which OPLs need a biopsy and to select a biopsy site. We developed a multimodal optical imaging system (MMIS) that fully integrates the acquisition, display, and analysis of macroscopic white-light (WL), autofluorescence (AF), and high-resolution microendoscopy (HRME) images to noninvasively evaluate OPLs. WL and AF images identify suspicious regions with high sensitivity, which are explored at higher resolution with the HRME to improve specificity. Key features include a heat map that delineates suspicious regions according to AF images, and real-time image analysis algorithms that predict pathologic diagnosis at imaged sites. Representative examples from ongoing studies of the MMIS demonstrate its ability to identify high-grade dysplasia in OPLs that are not clinically suspicious, and to avoid unnecessary biopsies of benign OPLs that are clinically suspicious. The MMIS successfully integrates optical imaging approaches (WL, AF, and HRME) at multiple scales for the noninvasive evaluation of OPLs.
Keywords: autofluorescence; fiber bundle; in vivo imaging; oral cancer; oral lesion.
Figures
References
-
- Ferlay J., et al. , “GLOBOCAN 2012 v1.0, cancer incidence and mortality worldwide: IARC CancerBase No. 11,” International Agency for Research on Cancer, Lyon, France, 2013, http://globocan.iarc.fr/Default.aspx (13 November 2016).
-
- Macey R., et al. , “Diagnostic tests for oral cancer and potentially malignant disorders in patients presenting with clinically evident lesions,” in Cochrane Database of Systematic Reviews, Macey R., Ed., p. 4, John Wiley and Sons, Ltd., Hoboken, New Jersey: (2015). - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
