

Safety and efficiency of a common and simplified protocol for pacemaker and defibrillator surveillance based on remote monitoring only: a long-term randomized trial (RM-ALONE)
- PMID: 30793735
- PMCID: PMC6568206
- DOI: 10.1093/eurheartj/ehz067
Safety and efficiency of a common and simplified protocol for pacemaker and defibrillator surveillance based on remote monitoring only: a long-term randomized trial (RM-ALONE)
Abstract
Aims: This trial aimed to evaluate the safety and efficiency of a common and simplified protocol for the surveillance of cardiac implantable electronic devices based on remote monitoring (RM) in patients with pacemakers (PMs) and implantable cardiac defibrillators (ICDs) for at least 24 months.
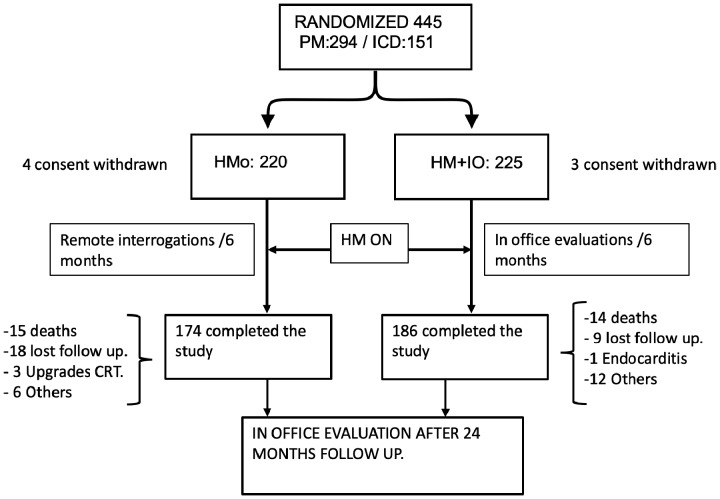
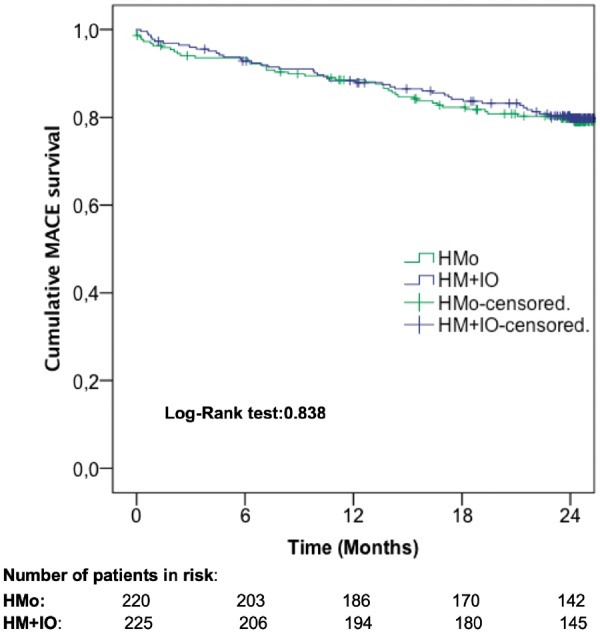
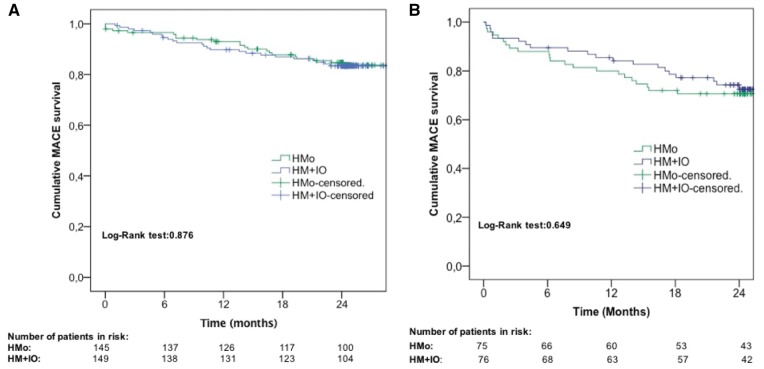
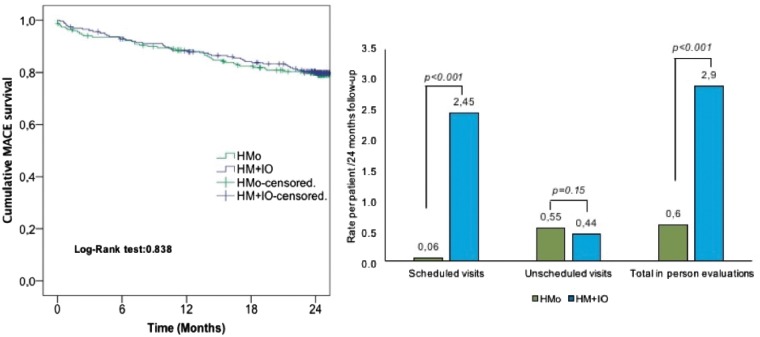
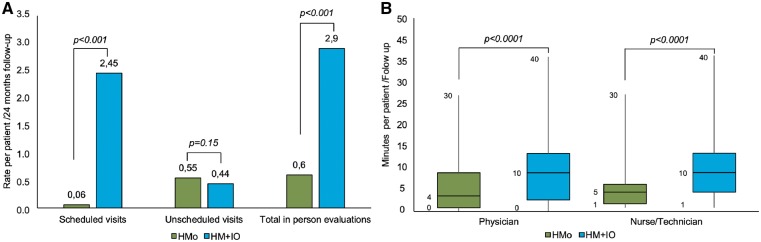
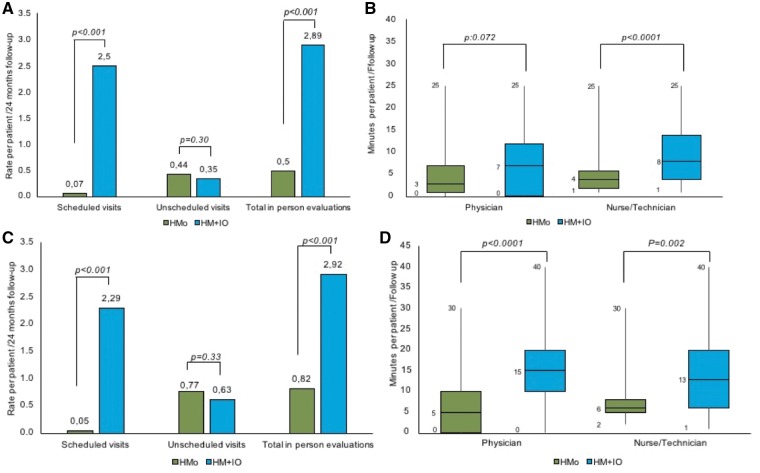
Methods and results: The RM-ALONE is a multicentre prospective trial that randomly assigned 445 patients in two groups, both followed by RM: the home monitoring-only (HMo) based on RM + remote interrogations (RIs) every 6 months and the HM + IO that adds in-office evaluations every 6 months to RM. Four hundred and forty-five patients were enrolled in the study, 294 PMs and 151 ICDs recipients. In the HMo group, 20% of patients experienced ≥1 major adverse cardiac event (MACE) vs. 19.5% in HM + IO group (P = 0.006 for non-inferiority). The proportion of patients with a PM/ICD who experienced ≥1 MACE was 15.2/29.3% in HMo group and 16.1/26.3% in HM + IO group (hazard ratio 0.95/1.15, 95% confidence interval 0.53-1.70/0.62-2.10). There were 789 in-office evaluations (136 in the HMo and 653 in the HM + IO; P < 0.001). There was a 79.2% reduction of in-office evaluations with no significant differences in unscheduled visits between groups: 122 (54.5%) in HMo and 101 (45.3%) in HM + IO; P = 0.15. The time a physician/nurse spent per patient/follow-up was significantly reduced in the HMo group: 4/5 min (0-30)/(1-30) vs. 10/10 min (0-40)/(1-40) in HM + IO (P < 0.0001).
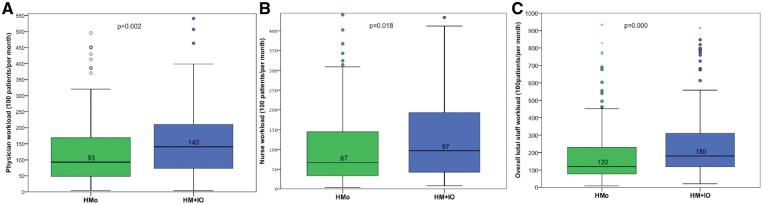
Conclusion: The RM-ALONE protocol common for ICD and PM surveillance, consisting of RM + RI every 6 months has proven safe and efficient in reducing hospital visits and staff workload.
Keywords: Implantable cardiac defibrillator; Pacemaker; Remote interrogation; Remote monitoring; Telemedicine.
© The Author(s) 2019. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
Comment in
-
Remote monitoring, healthcare costs, and workload for healthcare professionals.Eur Heart J. 2019 Jun 14;40(23):1847-1849. doi: 10.1093/eurheartj/ehz101. Eur Heart J. 2019. PMID: 30838393 No abstract available.
References
-
- Deering TF, Clair WK, Delaughter MC, Fisher WG, Garlitski AC, Wilkoff BL, Gillis AM.. A Heart Rhythm Society Electrophysiology Workforce study: current survey analysis of physician workforce trends. Heart Rhythm 2010;7:1346–1355. - PubMed
-
- Ricci RP, Morichelli L, Santini M.. Home monitoring remote control of pacemaker and implantable cardioverter defibrillator patients in clinical practice: impact on medical management and health-care resource utilization. Europace 2008;10:164–170. - PubMed
-
- Vogtmann T, Stiller S, Marek A, Kespohl S, Gomer M, Kuhlkamp V, Zach G, Loscher S, Baumann G.. Workload and usefulness of daily, centralized home monitoring for patients treated with CIEDs: results of the MoniC (Model Project Monitor Centre) prospective multicentre study. Europace 2013;15:219–226. - PubMed
-
- Varma N, Epstein AE, Irimpen A, Schweikert R, Love C; TRUST Investigators. Efficacy and safety of automatic remote monitoring for implantable cardioverter-defibrillator follow-up: the Lumos-T Safely Reduces Routine Office Device Follow-up (TRUST) trial. Circulation 2010;122:325–332. - PubMed
-
- Guedon-Moreau L, Lacroix D, Sadoul N, Clementy J, Kouakam C, Hermida JS, Aliot E, Boursier M, Bizeau O, Kacet S; ECOST trial Investigators. A randomized study of remote follow-up of implantable cardioverter defibrillators: safety and efficacy report of the ECOST trial. Eur Heart J 2013;34:605–614. - PMC - PubMed
