

What Is the Success of Repeat Surgical Treatment of a Local Recurrence After Initial Wide Resection of Soft Tissue Sarcomas?
- PMID: 30794216
- PMCID: PMC6259807
- DOI: 10.1007/s11999.0000000000000158
What Is the Success of Repeat Surgical Treatment of a Local Recurrence After Initial Wide Resection of Soft Tissue Sarcomas?
Abstract
Background: Treatment for patients with locally recurrent soft tissue sarcomas after wide resection is challenging, and few studies have examined the results of treating these patients. In treatment of recurrent tumors, it has been reported that positive margins are correlated to local rerecurrence, but the relationship between surgical margin and survival remains controversial and risk factors for local recurrences after wide resection of soft tissue sarcomas are not well established. This study examined clinical outcomes and factors associated with survival and local rerecurrence in patients with local recurrence after initial surgical treatment who underwent another resection with a goal of negative margins.
Questions/purposes: The purpose of this study was to determine (1) oncologic outcomes (survival rates and local rerecurrence-free rates) of surgical treatment for patients with local recurrence after wide resection; (2) whether factors associated with survival and local rerecurrence-free rates can be determined; and (3) the proportion of patients treated by amputation at final followup.
Methods: Between 1992 and 2013, we treated 530 patients with soft tissue sarcoma without metastasis. Of those, 26 (5%) were lost before 3 years of followup but were not known to have died. Of the remainder, 59 have had a local recurrence. Of those with a local recurrence, 34 (58%) were treated with wide resection, whereas 25 (42%) were treated with nonsurgical treatment including chemotherapy and radiotherapy. During that period, our general indications for wide resection were patients (1) without distant metastasis; or (2) without distant lymph node metastasis, and contraindications were distant organ metastasis and/or distant lymph node metastasis. Of those treated with wide resection, 30 (88%) were available for followup. We conducted a retrospective analysis of these 30 patients with local recurrence (17 men, 13 women) who had previously undergone wide resection. Patient followup ranged from 1 to 12 years (median, 5 years). Survivorship (including overall survival and survival free from repeat recurrence) was ascertained by the Kaplan-Meier method. Factors associated with survival were evaluated by the log-rank test. Amputations were performed when limb-sparing surgery was deemed unsuitable because of extensive involvement of the limb by tumor, including invasion of multiple muscle compartments and neurovascular components. Survivorship free from amputation was ascertained by the Kaplan-Meier method.
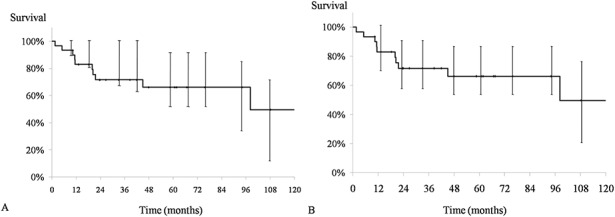
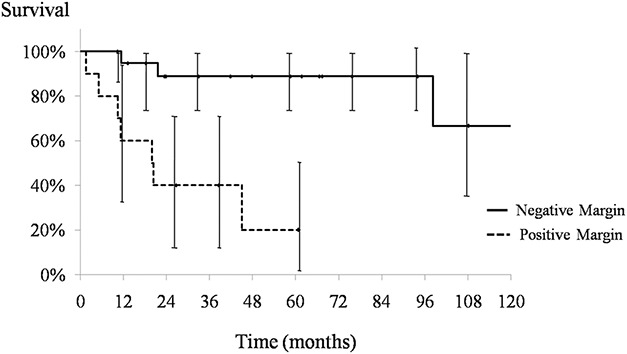
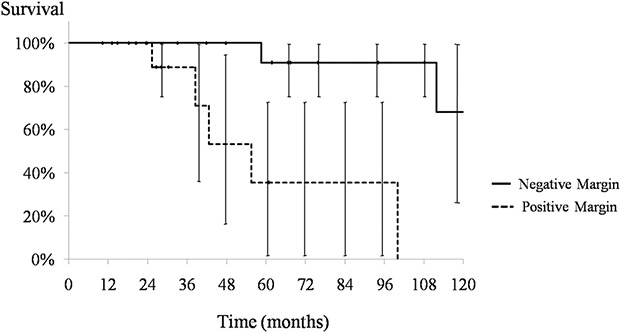
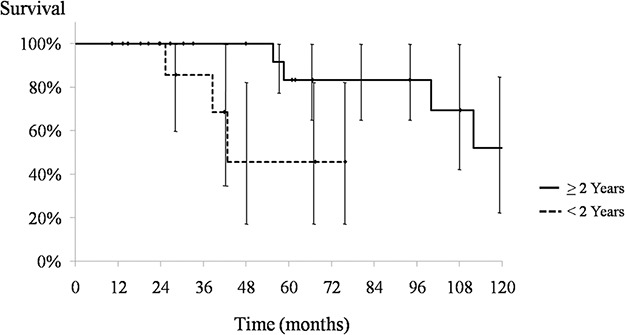
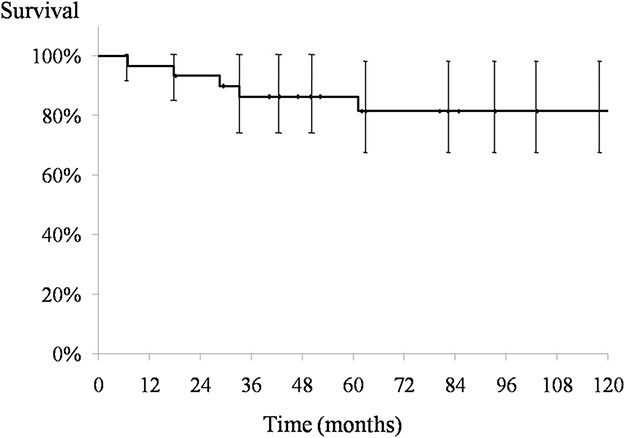
Results: Overall 5- and 10-year Kaplan-Meier survival rates after resection were 70% (95% confidence interval [CI], 50%-91%) and 44% (95% CI, 12%-76%), respectively, and 12 patients (40%) developed distant metastases after the second operation. Ten patients (33%) had additional local recurrences, and overall 5- and 10-year local rerecurrence-free rates were 66% (95% CI, 48%-85%) and 50% (95% CI, 18%-81%), respectively. A positive margin was associated with further recurrence (5-year local rerecurrence-free rates of positive margin: 20% [95% CI, 0%-52%], negative margin: 89% [95% CI, 74%-100%], p < 0.01) and with survival (5-year survival rates of positive margin: 36% [95% CI, 0%-75%], negative margin: 91% [95% CI, 74%-100%], p < 0.01). The survival rate was lower in patients with recurrence developing after 2 years (5-year survival rates of within 2 years: 46% [95% CI, 2%-90%], after 2 years: 83% [95% CI, 62%-100%], p = 0.01). The overall 5- and 10-year amputation-free rates were 86% (95% CI, 74%-99%) and 81% (95% CI, 67%-96%), respectively.
Conclusions: A surgical procedure with negative margins appears to be important for reducing the likelihood of local recurrences and improving survival of patients with rerecurrence after wide resection of soft tissue sarcomas. Although these findings need to be confirmed in larger studies, it appears that when tumor recurrence is evident within 2 years from the primary surgery, it is associated with a poor prognosis. Local recurrence within 2 years after wide resection may also be an indicator of aggressive tumor biology.
Level of evidence: Level IV, therapeutic study.
Conflict of interest statement
Each author certifies that neither he, nor any member of his immediate family, has funding or commercial associations (consultancies, stock ownership, equity interest, patent/licensing arrangements, etc) that might pose a conflict of interest in connection with the submitted article.
All ICMJE Conflict of Interest Forms for authors and
Figures
Comment in
-
CORR Insights®: What is the Success of Repeat Surgical Treatment of a Local Recurrence After Initial Wide Resection of Soft Tissue Sarcomas?Clin Orthop Relat Res. 2018 Sep;476(9):1801-1802. doi: 10.1097/01.blo.0000533636.35983.b7. Clin Orthop Relat Res. 2018. PMID: 29787395 Free PMC article. No abstract available.
Similar articles
-
Can Multistate Modeling of Local Recurrence, Distant Metastasis, and Death Improve the Prediction of Outcome in Patients With Soft Tissue Sarcomas?Clin Orthop Relat Res. 2017 May;475(5):1427-1435. doi: 10.1007/s11999-017-5232-x. Epub 2017 Jan 12. Clin Orthop Relat Res. 2017. PMID: 28083752 Free PMC article.
-
Impact of resection margin on outcome in soft-tissue sarcomas of the extremities treated with limb-sparing surgery and postoperative radiotherapy.World J Surg Oncol. 2024 Apr 26;22(1):113. doi: 10.1186/s12957-024-03380-y. World J Surg Oncol. 2024. PMID: 38664776 Free PMC article.
-
[Soft tissue sarcoma of the upper extremities. Analysis of factors relevant for prognosis in 160 patients].Chirurg. 2012 Feb;83(2):143-52. doi: 10.1007/s00104-011-2124-6. Chirurg. 2012. PMID: 21695557 German.
-
Wide Resection of Extremity/Truncal Soft Tissue Sarcomas.Surg Clin North Am. 2022 Aug;102(4):551-565. doi: 10.1016/j.suc.2022.05.002. Epub 2022 Jun 24. Surg Clin North Am. 2022. PMID: 35952687 Review.
-
Foot and Ankle Soft Tissue Sarcomas-Treatment and Oncologic Outcomes: A Systematic Review of the Literature.Foot Ankle Int. 2023 Nov;44(11):1199-1207. doi: 10.1177/10711007231198516. Epub 2023 Sep 26. Foot Ankle Int. 2023. PMID: 37750365
Cited by
-
Re-excision after unplanned excision of soft tissue sarcoma: A systematic review and metanalysis. The rationale of systematic re-excision.J Orthop. 2021 May 14;25:244-251. doi: 10.1016/j.jor.2021.05.022. eCollection 2021 May-Jun. J Orthop. 2021. PMID: 34099954 Free PMC article. Review.
-
Intraoperative Localization Using an Implanted Radar Reflector Facilitates Resection of Non-Palpable Trunk and Extremity Sarcoma.Ann Surg Oncol. 2021 Jun;28(6):3366-3374. doi: 10.1245/s10434-020-09229-4. Epub 2020 Oct 18. Ann Surg Oncol. 2021. PMID: 33073344 Review.
-
Principles of Surgical Treatment of Soft Tissue Sarcomas.Cancers (Basel). 2025 Jan 25;17(3):401. doi: 10.3390/cancers17030401. Cancers (Basel). 2025. PMID: 39941773 Free PMC article. Review.
-
Machine learning approaches in non-contact autofluorescence spectrum classification.PLOS Digit Health. 2024 Oct 9;3(10):e0000602. doi: 10.1371/journal.pdig.0000602. eCollection 2024 Oct. PLOS Digit Health. 2024. PMID: 39383196 Free PMC article.
-
Evaluation of the efficacy of CT-guided 3D template-assisted 125I seed implantation in the treatment of unresectable STS: a multicenter retrospective study.Sci Rep. 2022 Mar 8;12(1):3731. doi: 10.1038/s41598-022-07729-9. Sci Rep. 2022. PMID: 35260674 Free PMC article.
References
-
- Bonvalot S, Levy A, Terrier P, Tzanis D, Bellefqih S, Le Cesne A, Le Péchoux C. Primary extremity soft tissue sarcomas: does local control impact survival? Ann Surg Oncol. 2017;24:194–201. - PubMed
-
- Brennan MF. Local recurrence in soft tissue sarcoma: more about the tumor, less about the surgeon. Ann Surg Oncol. 2007;14:1528–1529. - PubMed
-
- Eilber FC, Brennan MF, Riedel E, Alektiar KM, Antonescu CR, Singer S. Prognostic factors for survival in patients with locally recurrent extremity soft tissue sarcomas. Ann Surg Oncol. 2005;12:228–236. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
