

Etiology of Above-knee Amputations in the United States: Is Periprosthetic Joint Infection an Emerging Cause?
- PMID: 30794239
- PMCID: PMC6259848
- DOI: 10.1007/s11999.0000000000000166
Etiology of Above-knee Amputations in the United States: Is Periprosthetic Joint Infection an Emerging Cause?
Abstract
Background: Above-knee amputation (AKA) is a morbid procedure and is performed for a number of conditions. Although AKA is usually performed for dysvascular disease, trauma, and malignancy, AKA is also considered in patients who have failed multiple salvage attempts at treating periprosthetic joint infection (PJI) of TKA. Although aggressive measures are being taken to treat PJI, the huge volume of TKAs might result in a large number of AKAs being performed for PJI in the United States. However, the national trends in the incidence of AKAs from different etiologies and the relative contribution of different etiologies to AKA are yet to be studied.
Questions/purposes: (1) What are the temporal trends in the incidence of AKAs (from all causes) in the US population from 1998 to 2013? (2) What are the temporal trends in the incidence of AKAs by etiology (dysvascular disease, trauma, malignancy, and PJI)? (3) What are the temporal trends in the relative contribution of different etiologies to AKA?
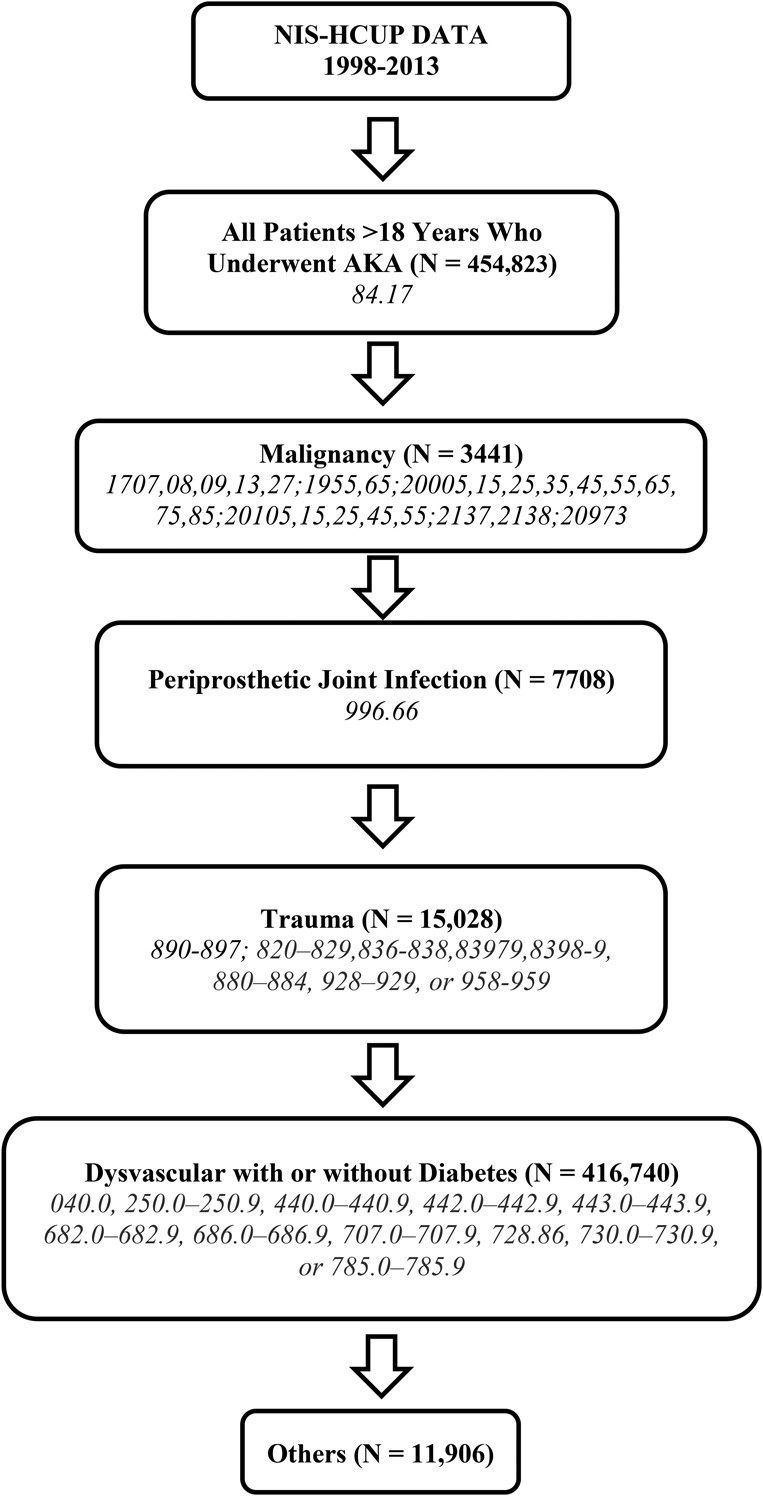
Methods: Using the Nationwide Inpatient Sample (NIS) from 1998 to 2013, AKAs were identified using International Classification of Diseases, 9 Revision (ICD-9) procedure code 84.17. The NIS database is the largest all-payer database in the United States containing information on approximately 20% of all the hospital admissions in the country. As a result of its sampling design, it allows for estimation of procedural volumes at the national level. All AKAs were grouped into one of the following five etiologies in a sequential manner using ICD-9 diagnosis codes: malignancy, PJI, trauma, dysvascular disease (peripheral vascular disease, diabetic, or a combination), and others. All of the numbers were converted to national estimates using sampling weights provided by the NIS, and the national incidence of AKAs resulting from various etiologies was calculated using the US population as the denominator. Poisson and linear regression analyses were used to analyze the annual trends.
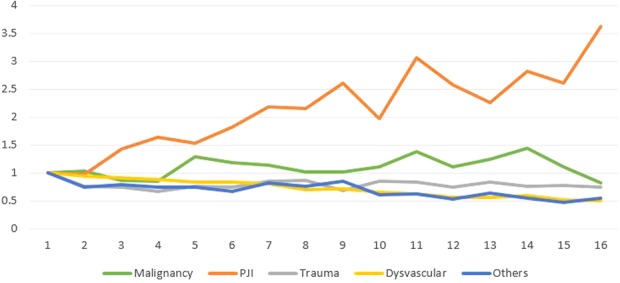
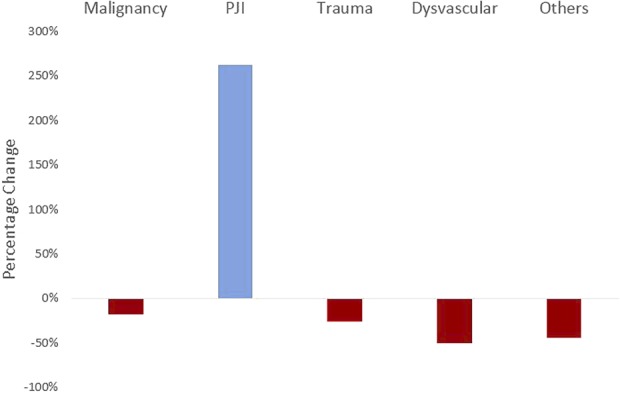
Results: From 1998 to 2013, the incidence of AKAs decreased by 47% from 174 to 92 AKAs per 1 million adults (incidence rate ratio [IRR]; change in the number of AKAs per 1 million adults per year; 0.96; 95% confidence interval [CI], 0.96-0.96; p < 0.001). The incidence of AKAs resulting from PJI increased by 263% (IRR, 1.07; 95% CI, 1.06-1.07; p < 0.001). An increase was also observed for AKAs from malignancy (IRR, 1.01; 95% CI, 1.00-1.02; p = 0.007), although to a smaller extent. AKAs from dysvascular causes (IRR, 0.96; 95% CI, 0.95-0.96; p < 0.001) and other etiologies (IRR, 0.97; 95% CI, 0.96-0.97; p < 0.001) decreased. There was no change in the incidence of AKAs related to trauma (IRR, 1.00; 95% CI, 0.99-1.00; p = 0.088). The proportion of AKAs resulting from PJI increased by 589% from 1998 to 2013 (coefficient = 0.18; 95% CI, 0.15-0.22; p < 0.001). The proportion of AKAs resulting from dysvascular causes decreased (coefficient = 0.18; 95% CI, 0.15-0.22; p < 0.001), whereas that resulting from malignancy (coefficient = 0.04; 95% CI, 0.03-0.05; p < 0.001) and trauma (coefficient = 0.13; 95% CI, 0.09-0.18; p < 0.001) increased.
Conclusions: The incidence of AKAs has decreased in the United States. AKAs related to dysvascular disease and other etiologies such as trauma and malignancy have either substantially decreased or remained fairly constant, whereas that resulting from PJI more than tripled. Given the increased resource utilization associated with limb loss, the results of this study suggest that national efforts to reduce disability should prioritize PJI. Further studies are required to evaluate the risk factors for AKA from PJI and to formulate better strategies to manage PJI.
Level of evidence: Level III, therapeutic study.
Conflict of interest statement
Each author certifies that neither he or she, nor any member of his or her immediate family, has funding or commercial associations (consultancies, stock ownership, equity interest, patent/licensing arrangements, etc) that might pose a conflict of interest in connection with the submitted article.
All ICMJE Conflict of Interest Forms for authors and
Figures
Comment in
-
CORR Insights®: Etiology of Above-knee Amputations in the United States: Is Periprosthetic Joint Infection an Emerging Cause?Clin Orthop Relat Res. 2018 Oct;476(10):1961-1963. doi: 10.1007/s11999.0000000000000274. Clin Orthop Relat Res. 2018. PMID: 29601394 Free PMC article. No abstract available.
Similar articles
-
Socioeconomic Status Is Associated with Risk of Above-knee Amputation After Periprosthetic Joint Infection of the Knee.Clin Orthop Relat Res. 2019 Jul;477(7):1531-1536. doi: 10.1097/CORR.0000000000000634. Clin Orthop Relat Res. 2019. PMID: 31210644 Free PMC article.
-
What Are the Frequency, Associated Factors, and Mortality of Amputation and Arthrodesis After a Failed Infected TKA?Clin Orthop Relat Res. 2017 Dec;475(12):2905-2913. doi: 10.1007/s11999-017-5285-x. Clin Orthop Relat Res. 2017. PMID: 28236080 Free PMC article.
-
Is Patient-reported Penicillin Allergy Independently Associated with Increased Risk of Prosthetic Joint Infection After Total Joint Arthroplasty of the Hip, Knee, and Shoulder?Clin Orthop Relat Res. 2020 Dec;478(12):2699-2709. doi: 10.1097/CORR.0000000000001497. Clin Orthop Relat Res. 2020. PMID: 33027190 Free PMC article.
-
Strategies for Management of Periprosthetic Joint Infection.Bull Hosp Jt Dis (2013). 2018 Mar;76(1):55-61. Bull Hosp Jt Dis (2013). 2018. PMID: 29537958 Review.
-
What Markers Best Guide the Timing of Reimplantation in Two-stage Exchange Arthroplasty for PJI? A Systematic Review and Meta-analysis.Clin Orthop Relat Res. 2018 Oct;476(10):1972-1983. doi: 10.1097/01.blo.0000534680.87622.43. Clin Orthop Relat Res. 2018. PMID: 30794241 Free PMC article.
Cited by
-
[PJI-TNM as new classification system for periprosthetic joint infections : An evaluation of 20 cases].Orthopade. 2021 Mar;50(3):198-206. doi: 10.1007/s00132-020-03933-5. Orthopade. 2021. PMID: 32533215 Free PMC article. German.
-
Outcomes of Total Knee Arthroplasty in Patients With a Prior Contralateral Above-Knee Amputation: A Retrospective Review of a Nationwide Database.Arthroplast Today. 2022 Feb 3;14:36-39. doi: 10.1016/j.artd.2021.10.022. eCollection 2022 Apr. Arthroplast Today. 2022. PMID: 35169600 Free PMC article. Review.
-
Symmetry Function: The Differences between Active and Non-Active Above-the-Knee Amputees.Sensors (Basel). 2022 Aug 9;22(16):5933. doi: 10.3390/s22165933. Sensors (Basel). 2022. PMID: 36015694 Free PMC article.
-
Socioeconomic Status Is Associated with Risk of Above-knee Amputation After Periprosthetic Joint Infection of the Knee.Clin Orthop Relat Res. 2019 Jul;477(7):1531-1536. doi: 10.1097/CORR.0000000000000634. Clin Orthop Relat Res. 2019. PMID: 31210644 Free PMC article.
-
CORR Insights®: Etiology of Above-knee Amputations in the United States: Is Periprosthetic Joint Infection an Emerging Cause?Clin Orthop Relat Res. 2018 Oct;476(10):1961-1963. doi: 10.1007/s11999.0000000000000274. Clin Orthop Relat Res. 2018. PMID: 29601394 Free PMC article. No abstract available.
References
-
- Agency for Healthcare Research & Quality. HCUPnet: a tool for identifying, tracking, and analyzing national hospital statistics. 2017. Available at: http://hcupnet.ahrq.gov/. Accessed July 23, 2017.
-
- Buller LT, Sabry FY, Easton RW, Klika AK, Barsoum WK. The preoperative prediction of success following irrigation and débridement with polyethylene exchange for hip and knee prosthetic joint infections. J Arthroplasty. 2012;27:857–864.4. - PubMed
-
- Burger H, Marincek C, Isakov E. Mobility of persons after traumatic lower limb amputation. Disabil Rehabil. 1997;19:272–277. - PubMed
-
- Cutson TM, Bongiorni DR. Rehabilitation of the older lower limb amputee: a brief review. J Am Geriatr Soc. 1996;44:1388–1393. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
