

Cost-effectiveness Analysis of Bariatric Surgery for Patients With Nonalcoholic Steatohepatitis Cirrhosis
- PMID: 30794300
- PMCID: PMC6484583
- DOI: 10.1001/jamanetworkopen.2019.0047
Cost-effectiveness Analysis of Bariatric Surgery for Patients With Nonalcoholic Steatohepatitis Cirrhosis
Abstract
Importance: Obesity is the most common risk factor for nonalcoholic steatohepatitis (NASH), the progressive form of nonalcoholic fatty liver disease that can lead to cirrhosis and hepatocellular carcinoma. Weight loss can be an effective treatment for obesity and may slow the progression of advanced liver disease.
Objective: To assess the cost-effectiveness of bariatric surgery in patients with NASH and compensated cirrhosis.
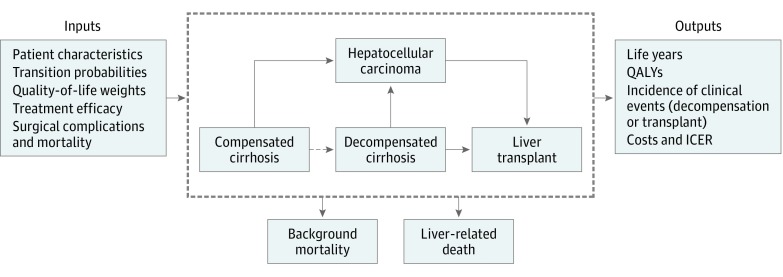
Design, setting, and participants: This economic evaluation study used a Markov-based state-transition model to simulate the benefits and risks of laparoscopic sleeve gastrectomy (SG), laparoscopic Roux-en-Y gastric bypass (GB), and intensive lifestyle intervention (ILI) compared with usual care in patients with NASH and compensated cirrhosis and varying baseline weight (overweight, mild obesity, moderate obesity, and severe obesity). Patients faced varied risks of perioperative mortality and complications depending on the type of surgery they underwent. Data were collected on March 22, 2017.
Main outcomes and measures: Life-years, quality-adjusted life-years (QALYs), costs (in 2017 $US), and incremental cost-effectiveness ratios (ICERs) were calculated.
Results: Demographic characteristics of the patient population were based on a previously published prospective study (n = 161). Patients in the model were 41.0% female, and the base case age was 54 years. Compared with usual care, SG was associated with an increase in QALYs of 0.263 to 1.180 (bounds of ranges represent overweight to severe obesity); GB, 0.263 to 1.207; and ILI, 0.004 to 0.216. Sleeve gastrectomy was also associated with an increase in life-years of 0.693 to 1.930; GB, 0.694 to 1.947; and ILI, 0.012 to 0.114. With usual care, expected life-years in overweight, mild obesity, moderate obesity, and severe obesity were 12.939, 11.949, 10.976, and 10.095, respectively. With usual care, QALY in overweight was 6.418; mild obesity, 5.790; moderate obesity, 5.186; and severe obesity, 4.577. Sleeve gastrectomy was the most cost-effective option for patients across all weight classes assessed: ICER for SG in patients with overweight was $66 119 per QALY; mild obesity, $18 716 per QALY; moderate obesity, $10 274 per QALY; and severe obesity, $6563 per QALY. A threshold analysis on the procedure cost of GB found that for GB to be cost-effective, the cost of the surgery must be decreased from its baseline value of $28 734 by $4889 for mild obesity, by $3189 for moderate obesity, and by $2289 for severe obesity. In overweight patients, GB involved fewer QALYs than SG, and thus decreasing the cost of surgery would not result in cost-effectiveness.
Conclusions and relevance: Bariatric surgery could be highly cost-effective in patients with NASH compensated cirrhosis and obesity or overweight. The findings from this analysis suggest that it can inform clinical trials evaluating the effect of bariatric procedures in patients with NASH cirrhosis, including those with a lower body mass index.
Conflict of interest statement
Figures
Comment in
-
Considering Bariatric Surgery in Patients With Nonalcoholic Steatohepatitis-Worth the Risk.JAMA Netw Open. 2019 Feb 1;2(2):e190053. doi: 10.1001/jamanetworkopen.2019.0053. JAMA Netw Open. 2019. PMID: 30794294 No abstract available.
Similar articles
-
Bariatric surgery for nonalcoholic steatohepatitis: A clinical and cost-effectiveness analysis.Hepatology. 2017 Apr;65(4):1156-1164. doi: 10.1002/hep.28958. Epub 2017 Feb 21. Hepatology. 2017. PMID: 27880977 Clinical Trial.
-
Estimated Cost-effectiveness of Medical Therapy, Sleeve Gastrectomy, and Gastric Bypass in Patients With Severe Obesity and Type 2 Diabetes.JAMA Netw Open. 2022 Feb 1;5(2):e2148317. doi: 10.1001/jamanetworkopen.2021.48317. JAMA Netw Open. 2022. PMID: 35157054 Free PMC article.
-
Cost-effectiveness of Bariatric Surgery in Adolescents With Obesity.JAMA Surg. 2017 Feb 1;152(2):136-141. doi: 10.1001/jamasurg.2016.3640. JAMA Surg. 2017. PMID: 27784062
-
Bile Acid Signaling: Mechanism for Bariatric Surgery, Cure for NASH?Dig Dis. 2015;33(3):440-6. doi: 10.1159/000371699. Epub 2015 May 27. Dig Dis. 2015. PMID: 26045281 Free PMC article. Review.
-
Adaptation of cost-effectiveness analyses to a single country: the case of bariatric surgery for obesity and overweight.Swiss Med Wkly. 2018 Jun 12;148:w14626. doi: 10.4414/smw.2018.14626. eCollection 2018. Swiss Med Wkly. 2018. PMID: 29894556 Review.
Cited by
-
Survival and Cost-Effectiveness of Bariatric Surgery Among Patients With Obesity and Cirrhosis.JAMA Surg. 2025 Jun 1;160(6):645-655. doi: 10.1001/jamasurg.2025.0490. JAMA Surg. 2025. PMID: 40172871
-
Systematic Literature Review and Critical Appraisal of Health Economic Models Used in Cost-Effectiveness Analyses in Non-Alcoholic Steatohepatitis: Potential for Improvements.Pharmacoeconomics. 2020 May;38(5):485-497. doi: 10.1007/s40273-019-00881-7. Pharmacoeconomics. 2020. PMID: 31919793
-
Nonalcoholic fatty liver disease and type 2 diabetes: where do Diabetologists stand?Clin Diabetes Endocrinol. 2020 Jun 5;6:9. doi: 10.1186/s40842-020-00097-1. eCollection 2020. Clin Diabetes Endocrinol. 2020. PMID: 32518675 Free PMC article. Review.
-
Non-alcoholic fatty liver disease: Is surgery the best current option and can novel endoscopy play a role in the future?World J Hepatol. 2022 Sep 27;14(9):1704-1717. doi: 10.4254/wjh.v14.i9.1704. World J Hepatol. 2022. PMID: 36185721 Free PMC article. Review.
-
Endoscopic Balloon Dilation Is Cost-Effective for Crohn's Disease Strictures.Dig Dis Sci. 2022 Dec;67(12):5462-5471. doi: 10.1007/s10620-022-07420-z. Epub 2022 Mar 15. Dig Dis Sci. 2022. PMID: 35290570
References
-
- Musso G, Cassader M, Rosina F, Gambino R. Impact of current treatments on liver disease, glucose metabolism and cardiovascular risk in non-alcoholic fatty liver disease (NAFLD): a systematic review and meta-analysis of randomised trials. Diabetologia. 2012;55(4):885-904. doi:10.1007/s00125-011-2446-4 - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
