

Noninvasive Imaging Biomarker Identifies Small Airway Damage in Severe Chronic Obstructive Pulmonary Disease
- PMID: 30794432
- PMCID: PMC6727153
- DOI: 10.1164/rccm.201811-2083OC
Noninvasive Imaging Biomarker Identifies Small Airway Damage in Severe Chronic Obstructive Pulmonary Disease
Abstract
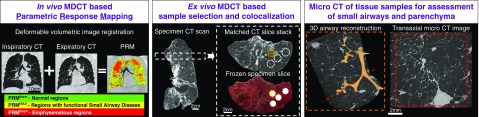
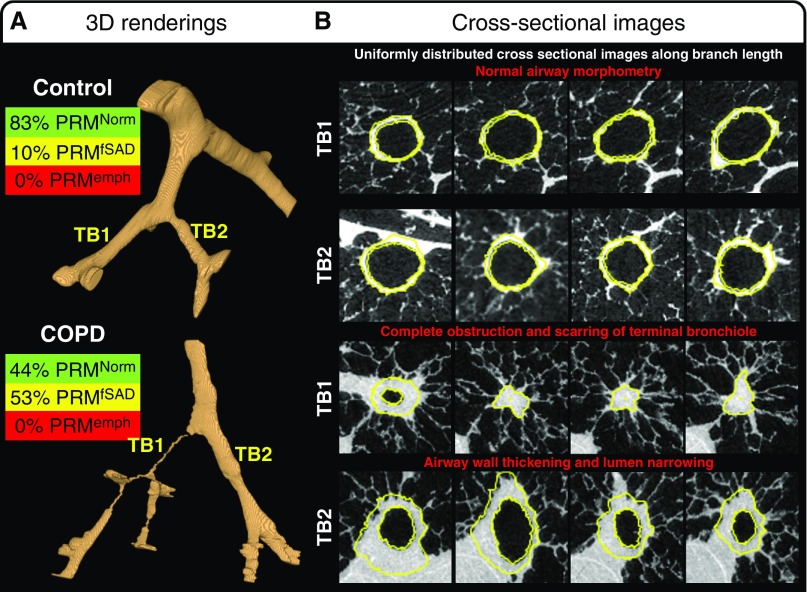
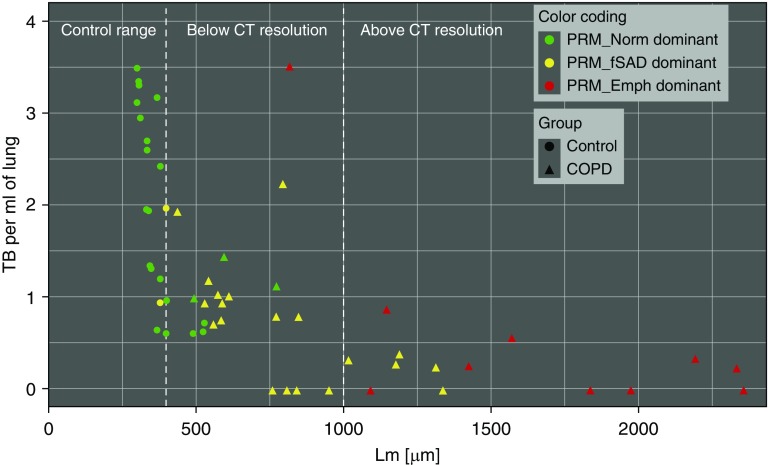
Rationale: Evidence suggests damage to small airways is a key pathologic lesion in chronic obstructive pulmonary disease (COPD). Computed tomography densitometry has been demonstrated to identify emphysema, but no such studies have been performed linking an imaging metric to small airway abnormality.Objectives: To correlate ex vivo parametric response mapping (PRM) analysis to in vivo lung tissue measurements of patients with severe COPD treated by lung transplantation and control subjects.Methods: Resected lungs were inflated, frozen, and systematically sampled, generating 33 COPD (n = 11 subjects) and 22 control tissue samples (n = 3 subjects) for micro-computed tomography analysis of terminal bronchioles (TBs; last generation of conducting airways) and emphysema.Measurements and Main Results: PRM analysis was conducted to differentiate functional small airways disease (PRMfSAD) from emphysema (PRMEmph). In COPD lungs, TB numbers were reduced (P = 0.01); surviving TBs had increased wall area percentage (P < 0.001), decreased circularity (P < 0.001), reduced cross-sectional luminal area (P < 0.001), and greater airway obstruction (P = 0.008). COPD lungs had increased airspace size (P < 0.001) and decreased alveolar surface area (P < 0.001). Regression analyses demonstrated unique correlations between PRMfSAD and TBs, with decreased circularity (P < 0.001), decreased luminal area (P < 0.001), and complete obstruction (P = 0.008). PRMEmph correlated with increased airspace size (P < 0.001), decreased alveolar surface area (P = 0.003), and fewer alveolar attachments per TB (P = 0.01).Conclusions: PRMfSAD identifies areas of lung tissue with TB loss, luminal narrowing, and obstruction. This is the first confirmation that an imaging biomarker can identify terminal bronchial pathology in established COPD and provides a noninvasive imaging methodology to identify small airway damage in COPD.
Keywords: COPD; airways disease; imaging; micro-CT.
Figures
Comment in
-
Validation of Imaging Measures in Chronic Obstructive Pulmonary Disease.Am J Respir Crit Care Med. 2019 Sep 1;200(5):524-525. doi: 10.1164/rccm.201902-0395ED. Am J Respir Crit Care Med. 2019. PMID: 30836008 Free PMC article. No abstract available.
-
Loss of Alveolar Attachments as a Pathomechanistic Link between Small Airway Disease and Emphysema.Am J Respir Crit Care Med. 2020 Apr 1;201(7):878-879. doi: 10.1164/rccm.201910-1981LE. Am J Respir Crit Care Med. 2020. PMID: 31804849 Free PMC article. No abstract available.
-
Reply to Janssen and Wouters: Loss of Alveolar Attachments as a Pathomechanistic Link between Small Airway Disease and Emphysema.Am J Respir Crit Care Med. 2020 Apr 1;201(7):879-880. doi: 10.1164/rccm.201911-2154LE. Am J Respir Crit Care Med. 2020. PMID: 31804850 Free PMC article. No abstract available.
References
-
- Rabe KF, Hurd S, Anzueto A, Barnes PJ, Buist SA, Calverley P, et al. Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med. 2007;176:532–555. - PubMed
-
- Vestbo J, Edwards LD, Scanlon PD, Yates JC, Agusti A, Bakke P, et al. ECLIPSE Investigators. Changes in forced expiratory volume in 1 second over time in COPD. N Engl J Med. 2011;365:1184–1192. - PubMed
-
- Koo HK, Vasilescu DM, Booth S, Hsieh A, Katsamenis OL, Fishbane N, et al. Small airways disease in mild and moderate chronic obstructive pulmonary disease: a cross-sectional study. Lancet Respir Med. 2018;6:591–602. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
