

Resistance towards metronidazole in Blastocystis sp.: A pathogenic consequence
- PMID: 30794628
- PMCID: PMC6386359
- DOI: 10.1371/journal.pone.0212542
Resistance towards metronidazole in Blastocystis sp.: A pathogenic consequence
Abstract
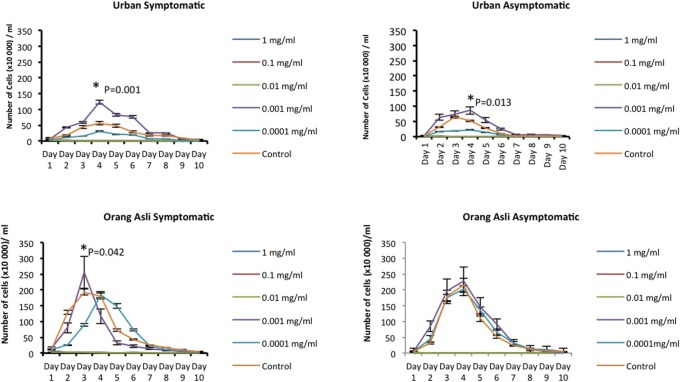
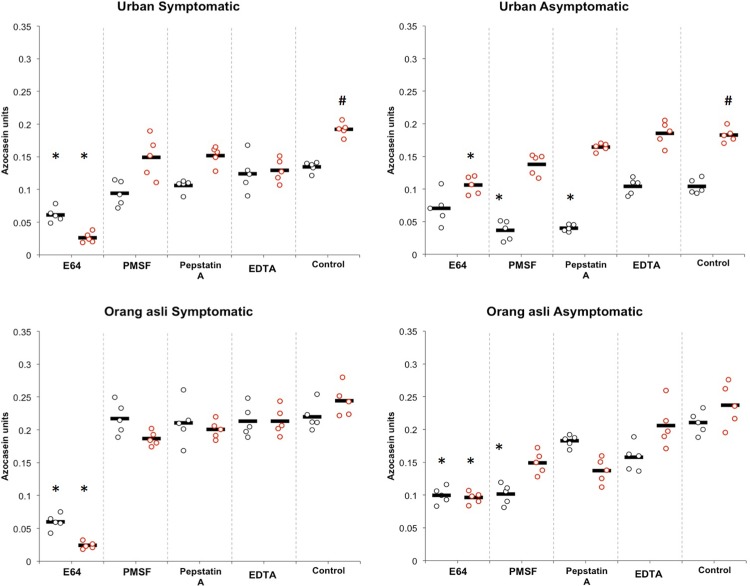
Blastocsytis sp. is a protozoan parasite that has been linked to common gastrointestinal illnesses. Metronidazole, the first line therapy, was reported to show frequent inefficacy. Previously, Blastocystis sp. isolated from different population showed varying metronidazole resistance. However, the effect of metronidazole treatment on pathogenic potentials of Blastocystis sp. isolated from different populations, which is known to have different gut environment, is unclear. This study investigates the in vitro effect of metronidazole on the pathogenic potentials of Blastocystis sp. isolated from urban and orang asli individuals. Blastocystis sp. ST 3 isolated from symptomatic and asymptomatic individuals were treated with a range of metronidazole concentration. The parasites' growth characteristics, apoptotic rate, specific protease activity and the ability to proliferate cancer cells were analyzed upon treatment with 0.001 mg/l metronidazole. The study demonstrates that Blastocystis sp. isolates showed increase in the parasite numbers especially the amoebic forms (only in urban isolates) after treating with metronidazole at the concentration of 0.001 mg/ml. High number of cells in post-treated isolates coincided with increase of apoptosis. There was a significant increase in cysteine protease of Blastocystis sp. isolates upon treatment despite the initial predominance of serine protease in asymptomatic isolates. Metronidazole resistant Blastocystis sp. also showed significant increase in cancer cell proliferation. Resistance to metronidazole did not show significant different influence on the pathogenicity between Blastocystis sp. isolated from urban and orang asli individual. However, an increase in parasite numbers, higher amoebic forms, cysteine protease and ability to proliferate cancer cells implicates a pathogenic role. The study provides evidence for the first time, the effect of metronidazole towards enhancing pathogenic potentials in Blastocystis sp. when isolated from different gut environment. This necessitates the need for reassessment of metronidazole treatment modalities.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures





Similar articles
-
Distinct Phenotypic Variation of Blastocystis sp. ST3 from Urban and Orang Asli Population-An Influential Consideration during Sample Collection in Surveys.Biology (Basel). 2022 Aug 12;11(8):1211. doi: 10.3390/biology11081211. Biology (Basel). 2022. PMID: 36009838 Free PMC article.
-
Higher amoebic and metronidazole resistant forms of Blastocystis sp. seen in schizophrenic patients.Parasit Vectors. 2022 Sep 5;15(1):313. doi: 10.1186/s13071-022-05418-0. Parasit Vectors. 2022. PMID: 36064639 Free PMC article.
-
Exacerbated symptoms in Blastocystis sp.-infected patients treated with metronidazole: two case studies.Parasitol Res. 2018 Aug;117(8):2585-2590. doi: 10.1007/s00436-018-5948-x. Epub 2018 Jun 5. Parasitol Res. 2018. PMID: 29872961
-
Eradication of Blastocystis carriage with antimicrobials: reality or delusion?J Clin Gastroenterol. 2010 Feb;44(2):85-90. doi: 10.1097/MCG.0b013e3181bb86ba. J Clin Gastroenterol. 2010. PMID: 19834337 Review.
-
Eradication of Blastocystis in humans: Really necessary for all?Parasitol Int. 2016 Dec;65(6 Pt B):797-801. doi: 10.1016/j.parint.2016.01.010. Epub 2016 Jan 15. Parasitol Int. 2016. PMID: 26780545 Review.
Cited by
-
The effects of LED Spectra on synthesis of antiparasitic bioactive compound in Eurycoma longifolia hairy root culture against Blastocystis Sp.Sci Rep. 2025 Apr 26;15(1):14662. doi: 10.1038/s41598-025-99906-9. Sci Rep. 2025. PMID: 40287563 Free PMC article.
-
In vitro susceptibility of human Blastocystis subtypes to simeprevir.Saudi J Biol Sci. 2021 Apr;28(4):2491-2501. doi: 10.1016/j.sjbs.2021.01.050. Epub 2021 Feb 2. Saudi J Biol Sci. 2021. PMID: 33935570 Free PMC article.
-
Antiprotozoal Effects of Pediococcus acidilactici-Derived Postbiotic on Blastocystis Subtypes ST1/ST3.Pathogens. 2025 Jul 5;14(7):664. doi: 10.3390/pathogens14070664. Pathogens. 2025. PMID: 40732711 Free PMC article.
-
Antiprotozoal potential of Salvadora persica against three virulent subtypes of Blastocystis sp.J Parasit Dis. 2020 Dec;44(4):694-701. doi: 10.1007/s12639-020-01247-z. Epub 2020 Jul 27. J Parasit Dis. 2020. PMID: 33184536 Free PMC article.
-
Influence of Proton Pump Inhibitors and Histamine Receptor 2 Antagonists on Blastocystis ST3 and Selected Microorganisms of Intestinal Microbiota In Vitro.Clin Transl Gastroenterol. 2021 Apr 9;12(4):e00325. doi: 10.14309/ctg.0000000000000325. Clin Transl Gastroenterol. 2021. PMID: 33835078 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
