

Emergency department triage prediction of clinical outcomes using machine learning models
- PMID: 30795786
- PMCID: PMC6387562
- DOI: 10.1186/s13054-019-2351-7
Emergency department triage prediction of clinical outcomes using machine learning models
Abstract
Background: Development of emergency department (ED) triage systems that accurately differentiate and prioritize critically ill from stable patients remains challenging. We used machine learning models to predict clinical outcomes, and then compared their performance with that of a conventional approach-the Emergency Severity Index (ESI).
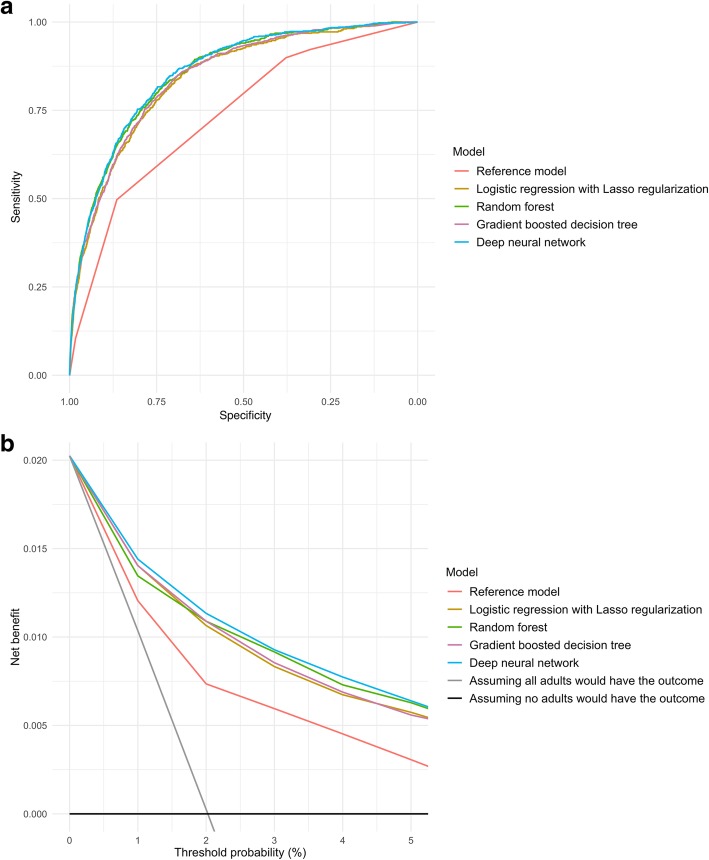
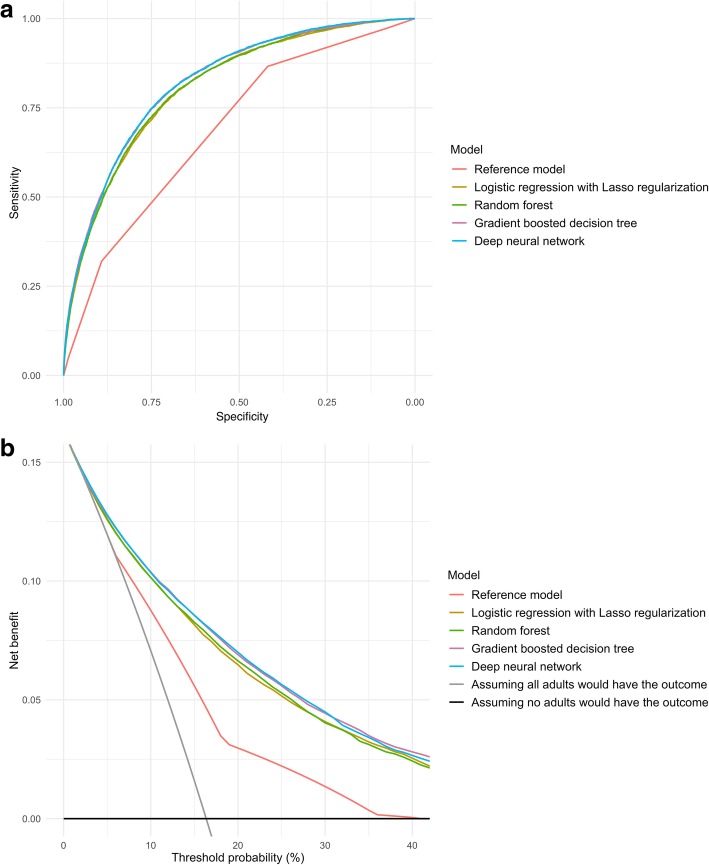
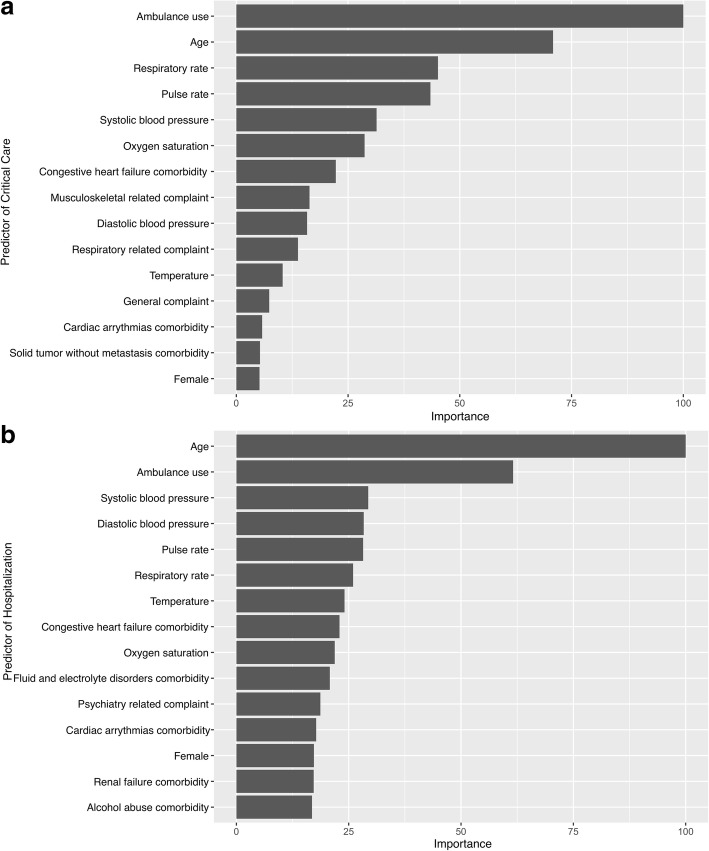
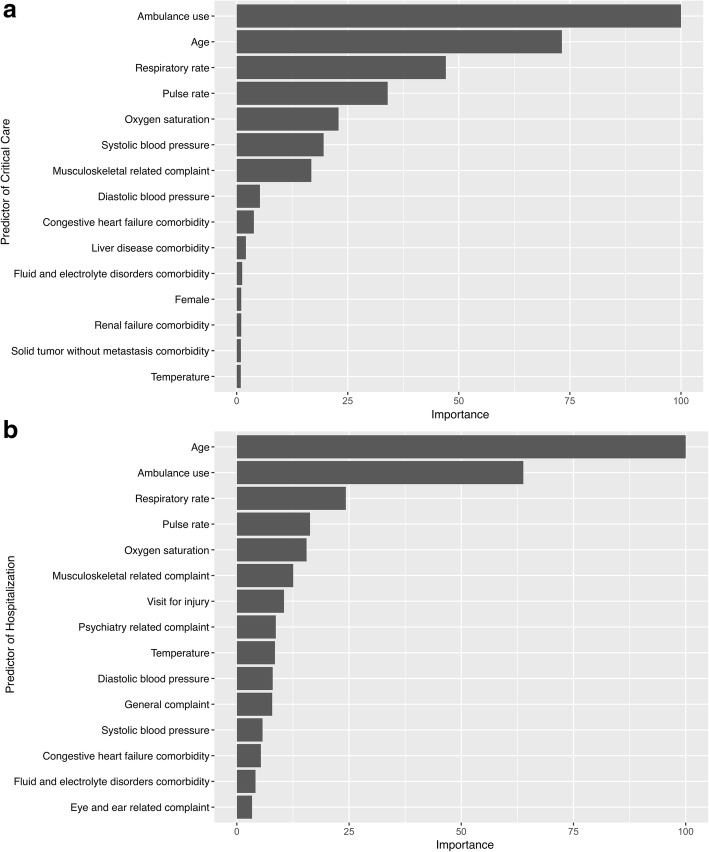
Methods: Using National Hospital and Ambulatory Medical Care Survey (NHAMCS) ED data, from 2007 through 2015, we identified all adult patients (aged ≥ 18 years). In the randomly sampled training set (70%), using routinely available triage data as predictors (e.g., demographics, triage vital signs, chief complaints, comorbidities), we developed four machine learning models: Lasso regression, random forest, gradient boosted decision tree, and deep neural network. As the reference model, we constructed a logistic regression model using the five-level ESI data. The clinical outcomes were critical care (admission to intensive care unit or in-hospital death) and hospitalization (direct hospital admission or transfer). In the test set (the remaining 30%), we measured the predictive performance, including area under the receiver-operating-characteristics curve (AUC) and net benefit (decision curves) for each model.
Results: Of 135,470 eligible ED visits, 2.1% had critical care outcome and 16.2% had hospitalization outcome. In the critical care outcome prediction, all four machine learning models outperformed the reference model (e.g., AUC, 0.86 [95%CI 0.85-0.87] in the deep neural network vs 0.74 [95%CI 0.72-0.75] in the reference model), with less under-triaged patients in ESI triage levels 3 to 5 (urgent to non-urgent). Likewise, in the hospitalization outcome prediction, all machine learning models outperformed the reference model (e.g., AUC, 0.82 [95%CI 0.82-0.83] in the deep neural network vs 0.69 [95%CI 0.68-0.69] in the reference model) with less over-triages in ESI triage levels 1 to 3 (immediate to urgent). In the decision curve analysis, all machine learning models consistently achieved a greater net benefit-a larger number of appropriate triages considering a trade-off with over-triages-across the range of clinical thresholds.
Conclusions: Compared to the conventional approach, the machine learning models demonstrated a superior performance to predict critical care and hospitalization outcomes. The application of modern machine learning models may enhance clinicians' triage decision making, thereby achieving better clinical care and optimal resource utilization.
Keywords: Critical care; Decision curve analysis; Emergency department; Hospital transfer; Hospitalization; Machine learning; Mortality; Prediction; Triage.
Conflict of interest statement
Ethics approval and consent to participate
The institutional review board of Massachusetts General Hospital waived review of this study.
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- HCUPnet. https://hcupnet.ahrq.gov Accessed 28 Nov 2018.
-
- Emergency department wait times, crowding and access. American College of Emergency Physicians News Room. http://newsroom.acep.org/2009-01-04-emergency-department-wait-times-crow... Accessed 1 Dec 2018.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
