

Discovering Associations Among Older Adults' Characteristics and Planned Nursing Interventions Using Electronic Health Record Data
- PMID: 30796148
- PMCID: PMC6847224
- DOI: 10.1891/1541-6577.33.1.58
Discovering Associations Among Older Adults' Characteristics and Planned Nursing Interventions Using Electronic Health Record Data
Abstract
Background and purpose: Little is known about how nursing assessments of strengths and signs/symptoms inform intervention planning in assisted living communities. The purpose of this study was to discover associations among older adults' characteristics and their planned nursing interventions.
Methods: This study employed a data-driven method, latent class analysis, using existing electronic health record data from a senior living community in the Midwest. A convenience sample comprised de-identified data of well-being assessments and care plans for 243 residents. Latent class analysis, descriptive, and inferential statistics were used to group the sample, summarize strengths and problems attributes, nursing interventions, and Knowledge, Behavior, and Status scores, and detect differences.
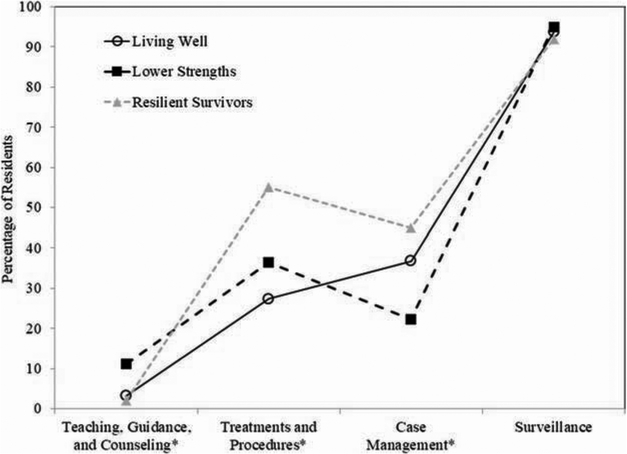
Results: Three groups presented based on patterns of strengths and signs/symptoms combined with problem concepts: Living Well (n = 95) had more strengths and fewer signs/symptoms; Lower Strengths (n = 99) had fewer strengths and more signs/symptoms; and Resilient Survivors (n = 49) had more strengths and more signs/symptoms. Some associations were found among group characteristics and planned interventions. Living Well had the lowest average number of planned interventions per resident (Mean = 2.7; standard deviation [SD] = 1.7) followed by Lower Strengths (Mean = 3.8; SD = 2.6) and Resilient Survivors (Mean = 4.1; SD = 3.4).
Implications for practice: This study offers new knowledge in the use of a strengths-based ontology to facilitate a nursing discourse that leverages use of older adults' strengths to address their problems and support their living a healthier life. It also offers the potential to complement the problem-based infrastructure in clinical practice and documentation.
Keywords: data-driven research; older adults; problems; strengths; the Omaha System.
© Copyright 2019 Springer Publishing Company, LLC.
Conflict of interest statement
Figures




Similar articles
-
Exploring Large Community- and Clinically-Generated Datasets to Understand Resilience Before and During the COVID-19 Pandemic.J Nurs Scholarsh. 2021 May;53(3):262-269. doi: 10.1111/jnu.12634. Epub 2021 Apr 3. J Nurs Scholarsh. 2021. PMID: 33811723 Free PMC article.
-
Exploring Older Adults' Strengths, Problems, and Wellbeing Using De-identified Electronic Health Record Data.AMIA Annu Symp Proc. 2018 Dec 5;2018:1263-1272. eCollection 2018. AMIA Annu Symp Proc. 2018. PMID: 30815168 Free PMC article.
-
Seeing the whole person: feasibility of using the Omaha System to describe strengths of older adults with chronic illness.Res Theory Nurs Pract. 2014;28(4):299-315. doi: 10.1891/1541-6577.28.4.299. Res Theory Nurs Pract. 2014. PMID: 25577860
-
Preventive home care of frail older people: a review of recent case management studies.J Clin Nurs. 2004 Sep;13(6B):112-20. doi: 10.1111/j.1365-2702.2004.01054.x. J Clin Nurs. 2004. PMID: 15724826 Review.
-
Iatrogenesis, frailty, and geriatric syndromes.Geriatr Nurs. 2010 Sep-Oct;31(5):368-74. doi: 10.1016/j.gerinurse.2010.08.004. Epub 2010 Sep 15. Geriatr Nurs. 2010. PMID: 20832910 Review.
Cited by
-
Disseminating Strengths-Oriented Best Practices in Diabetes Care Utilizing a Standardized Language within a Global Community.AMIA Annu Symp Proc. 2020 Mar 4;2019:448-456. eCollection 2019. AMIA Annu Symp Proc. 2020. PMID: 32308838 Free PMC article.
-
Exploring Large Community- and Clinically-Generated Datasets to Understand Resilience Before and During the COVID-19 Pandemic.J Nurs Scholarsh. 2021 May;53(3):262-269. doi: 10.1111/jnu.12634. Epub 2021 Apr 3. J Nurs Scholarsh. 2021. PMID: 33811723 Free PMC article.
-
Understanding Whole-Person Health and Resilience During the COVID-19 Pandemic and Beyond: A Cross-sectional and Descriptive Correlation Study.JMIR Nurs. 2022 May 16;5(1):e38063. doi: 10.2196/38063. JMIR Nurs. 2022. PMID: 35576563 Free PMC article.
References
-
- Agency for Healthcare Research and Quality. (2012). Prospects for care coordination measurement using electronic data sources (Publication No. 12–0014-EF). Washington, DC: AHRQ.
-
- American Medical Informatics Association (AMIA). (2017). Redefining our picture of health: Towards a person-centered integrated care, research, wellness, and community ecosystem. A white paper of the 2017 AMIA Policy Invitational; Retrieved from https://www.amia.org/sites/default/files/API-2017-White-Paper-Redefining...
-
- Banning M (2008). A review of clinical decision making: Models and current research. Journal of Clinical Nursing, 17(2), 187–95. - PubMed
-
- Das R (2015, August 11). A silver tsunami invades the health of nations. Forbes. Retrived from https://www.forbes.com/sites/reenitadas/2015/08/11/a-silver-tsunami-inva...
-
- Federal Interagency Forum on Aging-Related Statistics. (2016). Older Americans 2016: Key indicators of well-being. Federal Interagency Forum on Aging-Related Statistics. Washington, DC: U.S. Government Printing Office.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources