

Comparison between dynamic gadoxetate-enhanced MRI and 99mTc-mebrofenin hepatobiliary scintigraphy with SPECT for quantitative assessment of liver function
- PMID: 30796575
- PMCID: PMC6682576
- DOI: 10.1007/s00330-019-06029-7
Comparison between dynamic gadoxetate-enhanced MRI and 99mTc-mebrofenin hepatobiliary scintigraphy with SPECT for quantitative assessment of liver function
Abstract
Objectives: To compare Gd-EOB-DTPA dynamic hepatocyte-specific contrast-enhanced MRI (DHCE-MRI) with 99mTc-mebrofenin hepatobiliary scintigraphy (HBS) as quantitative liver function tests for the preoperative assessment of patients undergoing liver resection.
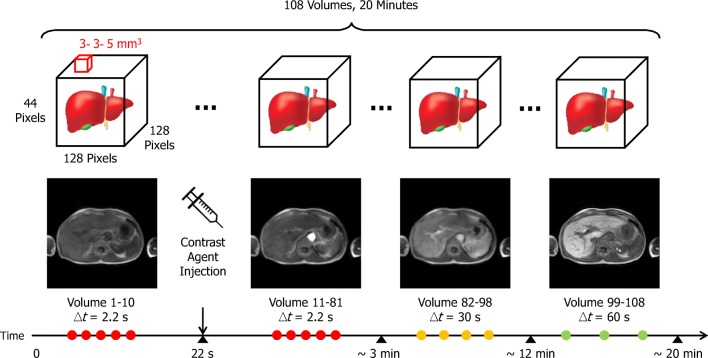
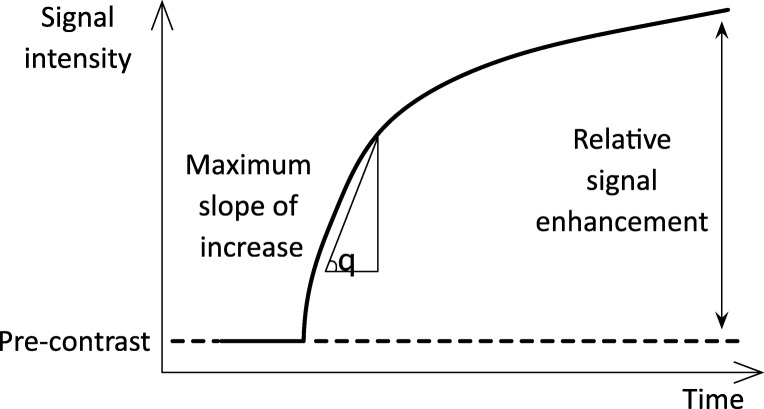
Methods: Patients undergoing liver surgery and preoperative assessment of future remnant liver (FRL) function using 99mTc-mebrofenin HBS were included. Patients underwent DHCE-MRI. Total liver uptake function was calculated for both modalities: mebrofenin uptake rate (MUR) and Ki respectively. The FRL was delineated with both SPECT-CT and MRI to calculate the functional share. Blood samples were taken to assess biochemical liver parameters.
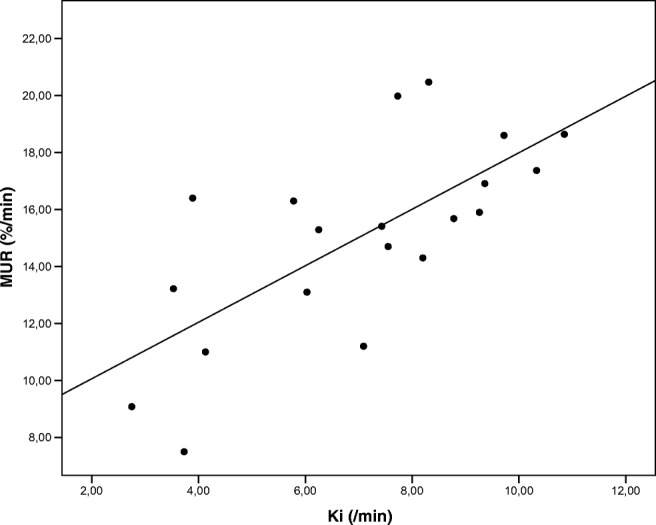
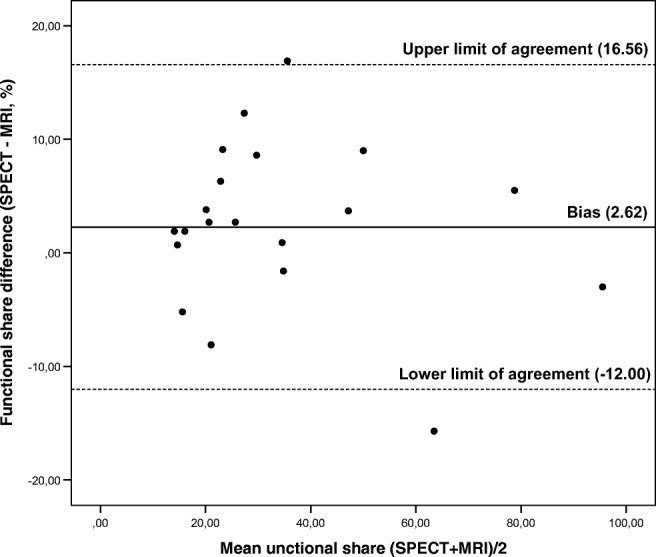
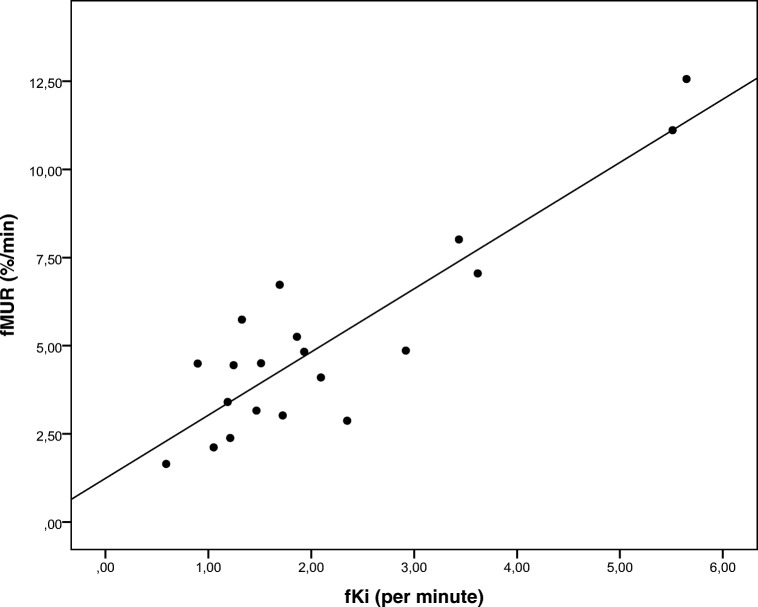
Results: A total of 20 patients were included. The HBS-derived MUR and the DHCE-MRI-derived mean Ki correlated strongly for both total and FRL function (Pearson r = 0.70, p = 0.001 and r = 0.89, p < 0.001 respectively). There was a strong agreement between the functional share determined with both modalities (ICC = 0.944, 95% CI 0.863-0.978, n = 20). There was a significant negative correlation between liver aminotransferases and bilirubin for both MUR and Ki.
Conclusions: Assessment of liver function with DHCE-MRI is comparable with that of 99mTc-mebrofenin HBS and has the potential to be combined with diagnostic MRI imaging. This can therefore provide a one-stop-shop modality for the preoperative assessment of patients undergoing liver surgery.
Key points: • Quantitative assessment of liver function using hepatobiliary scintigraphy is performed in the preoperative assessment of patients undergoing liver surgery in order to prevent posthepatectomy liver failure. • Gd-EOB-DTPA dynamic hepatocyte-specific contrast-enhanced MRI (DHCE-MRI) is an emerging method to quantify liver function and can serve as a potential alternative to hepatobiliary scintigraphy. • Assessment of liver function with dynamic gadoxetate-enhanced MRI is comparable with that of hepatobiliary scintigraphy and has the potential to be combined with diagnostic MRI imaging.
Keywords: Gadolinium ethoxybenzyl DTPA; Liver function tests; Magnetic resonance imaging; Technetium Tc 99m mebrofenin.
Conflict of interest statement
The authors of this manuscript declare no relationships with any companies, whose products or services may be related to the subject matter of the article.
Figures

References
-
- Belghiti J, Hiramatsu K, Benoist S, Massault PP, Sauvanet A, Farges O. Seven hundred forty-seven hepatectomies in the 1990s: an update to evaluate the actual risk of liver resection 11. No competing interests declared. J Am Coll Surg. 2000;191:38–46. doi: 10.1016/S1072-7515(00)00261-1. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
