

CT imaging findings of epiploic appendagitis: an unusual cause of abdominal pain
- PMID: 30796645
- PMCID: PMC6386757
- DOI: 10.1186/s13244-019-0715-9
CT imaging findings of epiploic appendagitis: an unusual cause of abdominal pain
Abstract
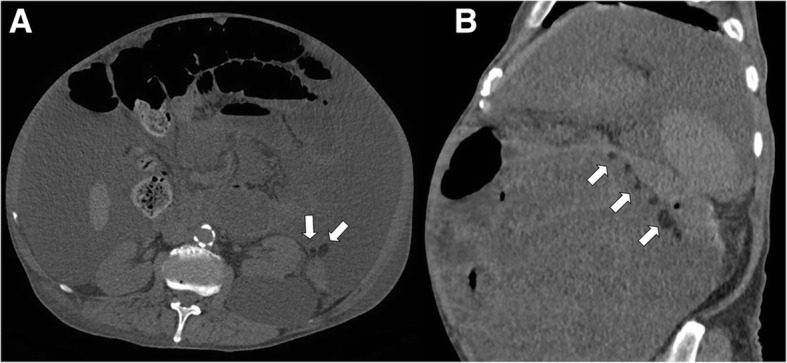
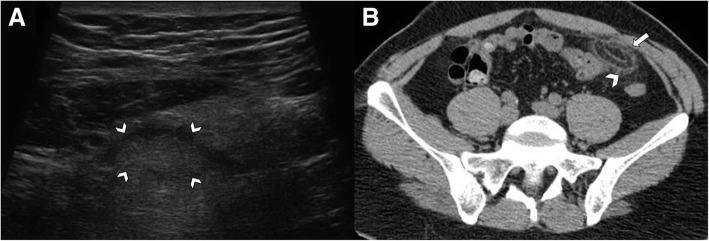
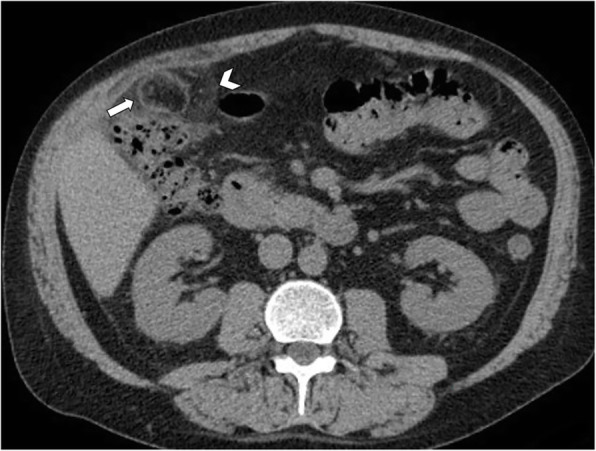
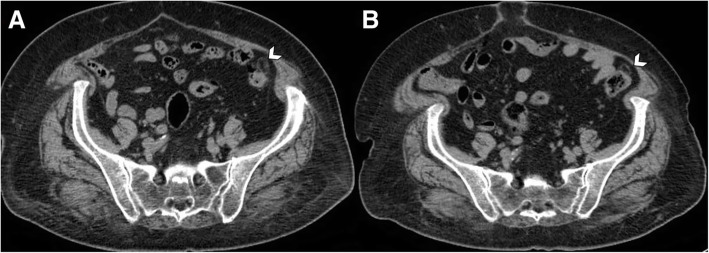
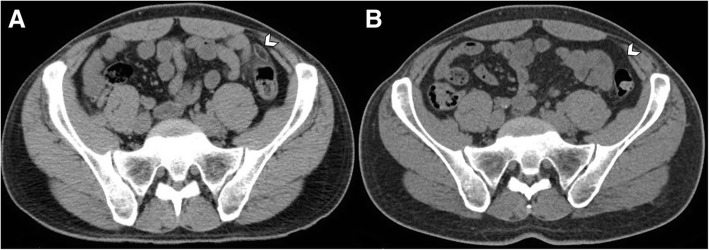
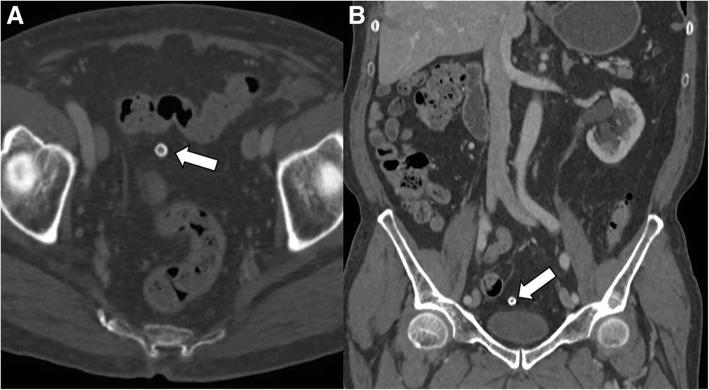
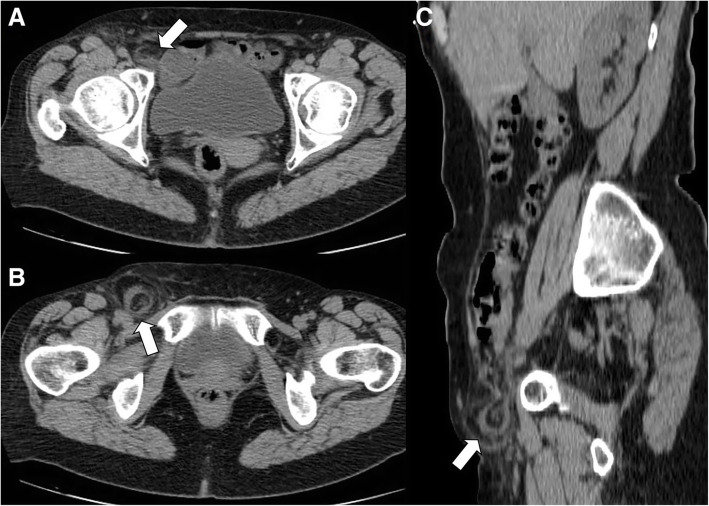
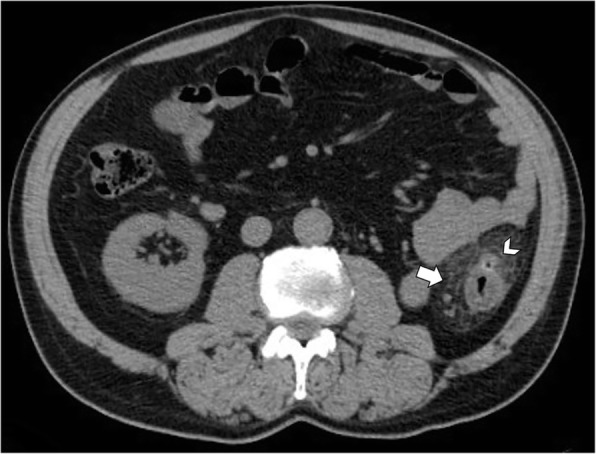
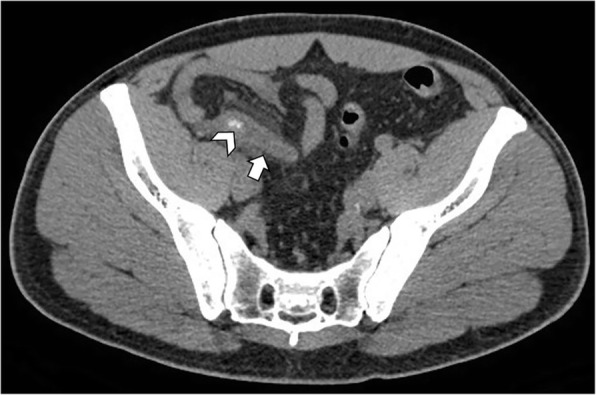
Epiploic appendagitis is a rare cause of acute abdominal pain, determined by a benign self-limiting inflammation of the epiploic appendages. It may manifest with heterogeneous clinical presentations, mimicking other more severe entities responsible of acute abdominal pain, such as acute diverticulitis or appendicitis. Given its importance as clinical mimicker, imaging plays a crucial role to avoid inaccurate diagnosis that may lead to unnecessary hospitalization, antibiotic therapy, and surgery. CT represents the gold standard technique for the evaluation of patients with indeterminate acute abdominal pain. Imaging findings include the presence of an oval lesion with fat-attenuation surrounded by a thin hyperdense rim on CT ("hyperattenuating ring sign") abutting anteriorly the large bowel, usually associated with inflammation of the adjacent mesentery. A central high-attenuation focus within the fatty lesion ("central dot sign") can sometimes be observed and is indicative of a central thrombosed vein within the inflamed epiploic appendage. Rarely, epiploic appendagitis may be located within a hernia sac or attached to the vermiform appendix. Chronically infarcted epiploic appendage may detach, appearing as an intraperitoneal loose calcified body in the abdominal cavity. In this review, we aim to provide an overview of the clinical presentation and key imaging features that may help the radiologist to make an accurate diagnosis and guide the clinical management of those patients.
Keywords: Abdominal pain; Acute abdomen; Adipose tissue; Differential diagnosis; Epiploic appendices; Large intestine.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures




References
-
- Singh AK, Gervais DA, Hahn PF, Sagar P, Mueller PR, Novelline RA. Acute epiploic Appendagitis and its mimics. Radiographics. 2005;25:1521–1534. - PubMed
-
- Almeida AT, Melão L, Viamonte B, Cunha R, Pereira JM. Epiploic appendagitis: an entity frequently unknown to clinicians—diagnostic imaging, pitfalls, and look-alikes. AJR Am J Roentgenol. 2009;193:1243–1251. - PubMed
-
- Schnedl WJ, Krause R, Tafeit E, Tillich M, Lipp RW, Wallner-Liebmann SJ. Insights into epiploic appendagitis. Nat Rev Gastroenterol Hepatol. 2011;8:45–49. - PubMed
-
- Pereira JM, Sirlin CB, Pinto PS, Jeffrey RB, Stella DL, Casola G. Disproportionate fat stranding: a helpful CT sign in patients with acute abdominal pain. Radiographics. 2004;24:703–715. - PubMed
-
- Ghahremani GG, White EM, Hoff FL, Gore RM, Miller JW, Christ ML. Appendices epiploicae of the colon: radiologic and pathologic features. Radiographics. 1992;12:59–77. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
