

Safety and Immunogenicity of a 2-Dose Heterologous Vaccination Regimen With Ad26.ZEBOV and MVA-BN-Filo Ebola Vaccines: 12-Month Data From a Phase 1 Randomized Clinical Trial in Uganda and Tanzania
- PMID: 30796818
- PMCID: PMC6548900
- DOI: 10.1093/infdis/jiz070
Safety and Immunogenicity of a 2-Dose Heterologous Vaccination Regimen With Ad26.ZEBOV and MVA-BN-Filo Ebola Vaccines: 12-Month Data From a Phase 1 Randomized Clinical Trial in Uganda and Tanzania
Abstract
Background: Ebola vaccine development was accelerated in response to the 2014 Ebola virus infection outbreak. This phase 1 study (VAC52150EBL1004) assessed safety, tolerability, and immunogenicity of heterologous 2-dose Ad26.ZEBOV, MVA-BN-Filo vaccination regimens in the Lake Victoria Basin of Tanzania and Uganda in mid-level altitude, malaria-endemic settings.
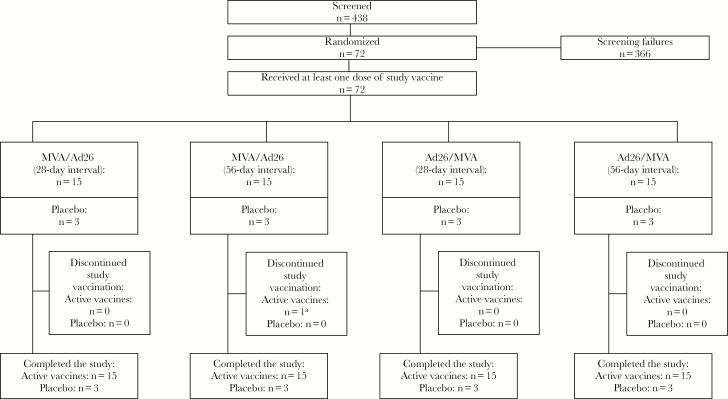
Methods: Healthy volunteers aged 18-50 years from Tanzania (n = 25) and Uganda (n = 47) were randomized to receive placebo or active vaccination with Ad26.ZEBOV or MVA-BN-Filo (first vaccination), followed by MVA-BN-Filo or Ad26.ZEBOV (second vaccination) dose 2, respectively, with intervals of 28 or 56 days.
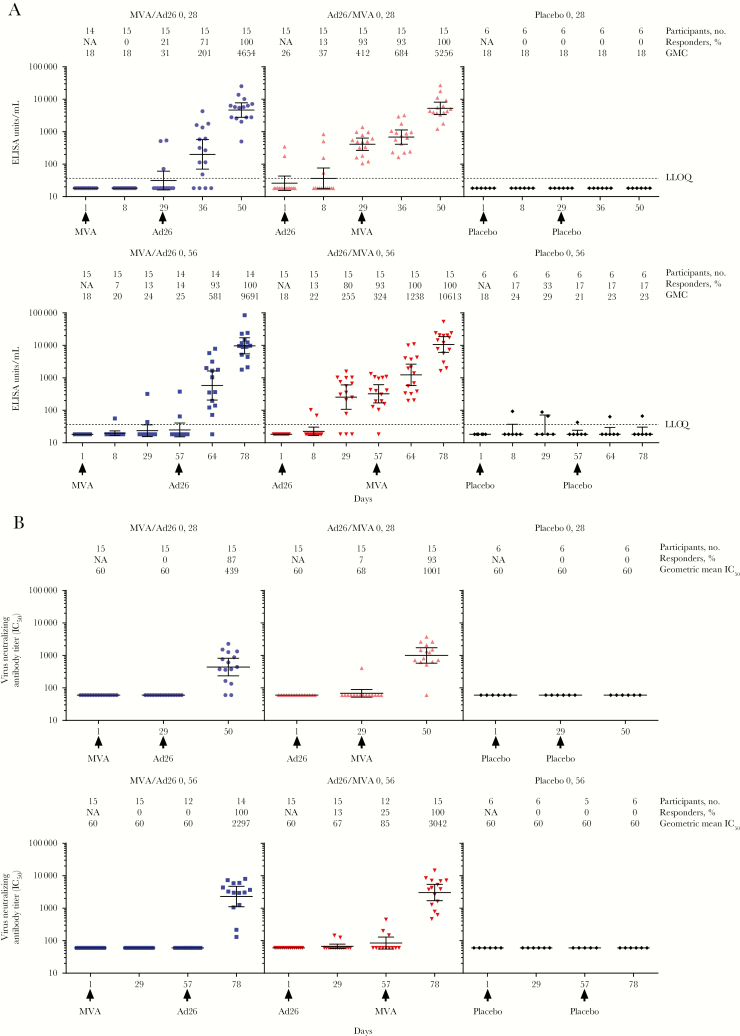
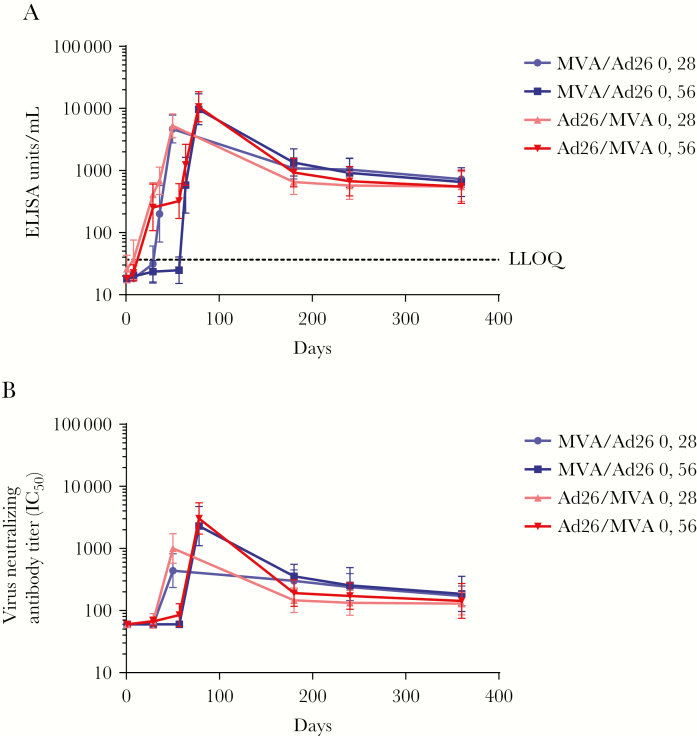
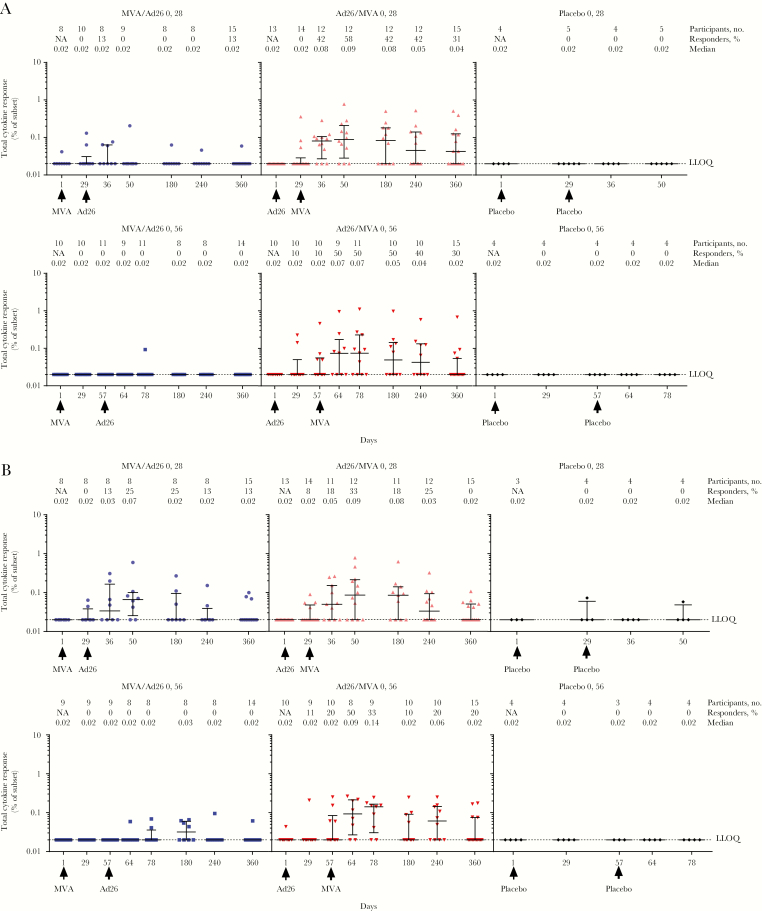
Results: Seventy-two adults were randomized to receive vaccine (n = 60) or placebo (n = 12). No vaccine-related serious adverse events were reported. The most frequent solicited local and systemic adverse events were injection site pain (frequency, 70%, 66%, and 42% per dose for MVA-BN-Filo, Ad26.ZEBOV, and placebo, respectively) and headache (57%, 56%, and 46%, respectively). Adverse event patterns were similar among regimens. Twenty-one days after dose 2, 100% of volunteers demonstrated binding antibody responses against Ebola virus glycoprotein, and 87%-100% demonstrated neutralizing antibody responses. Ad26.ZEBOV dose 1 vaccination induced more-robust initial binding antibody and cellular responses than MVA-BN-Filo dose 1 vaccination.
Conclusions: Heterologous 2-dose vaccination with Ad26.ZEBOV and MVA-BN-Filo against Ebola virus is well tolerated and immunogenic in healthy volunteers.
Clinical trials registration: NCT02376400.
Keywords: Ad26.ZEBOV; Ebola vaccine; MVA-BN-Filo; heterologous 2-dose; safety and immunogenicity.
© The Author(s) 2019. Published by Oxford University Press for the Infectious Diseases Society of America.
Figures
References
-
- Centers for Disease Control and Prevention (CDC). 2014 Ebola outbreak in West Africa - case counts 2016. https://www.cdc.gov/vhf/ebola/outbreaks/2014-west-africa/case-counts.html. Accessed April 2018.
-
- Centers for Disease Control and Prevention (CDC). Outbreaks chronology: Ebola virus disease 2015. https://www.cdc.gov/vhf/ebola/outbreaks/history/chronology.html. Accessed April 2018.
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
