

Deriving the optimal limit of detection for an HCV point-of-care test for viraemic infection: Analysis of a global dataset
- PMID: 30797050
- PMCID: PMC7014921
- DOI: 10.1016/j.jhep.2019.02.011
Deriving the optimal limit of detection for an HCV point-of-care test for viraemic infection: Analysis of a global dataset
Abstract
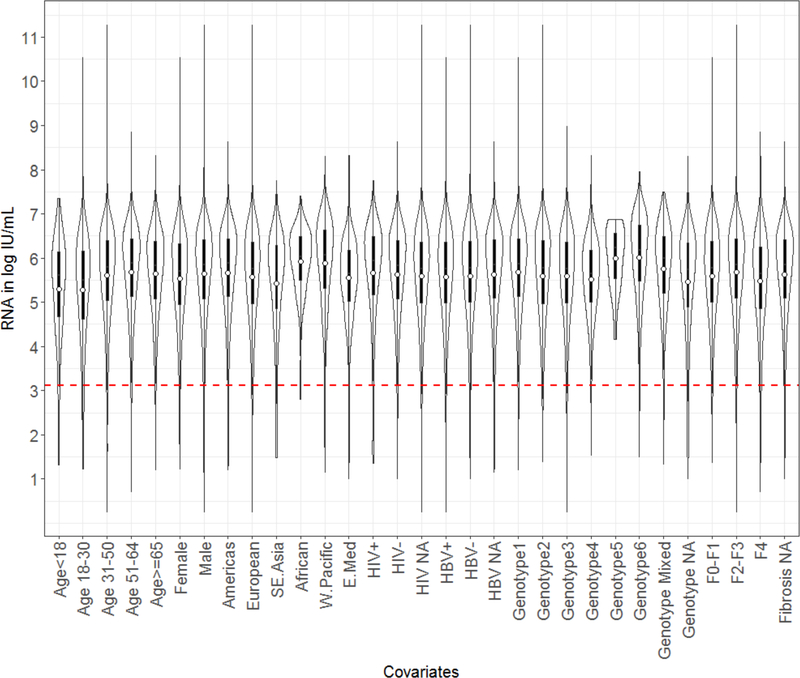
Background & aims: Affordable point-of-care tests for hepatitis C (HCV) viraemia are needed to improve access to treatment in low- and middle-income countries. Our aims were to determine the target limit of detection (LOD) necessary to diagnose the majority of people with HCV eligible for treatment, and identify characteristics associated with low-level viraemia (LLV) (defined as the lowest 3% of the distribution of HCV RNA) to understand those at risk of being misdiagnosed.
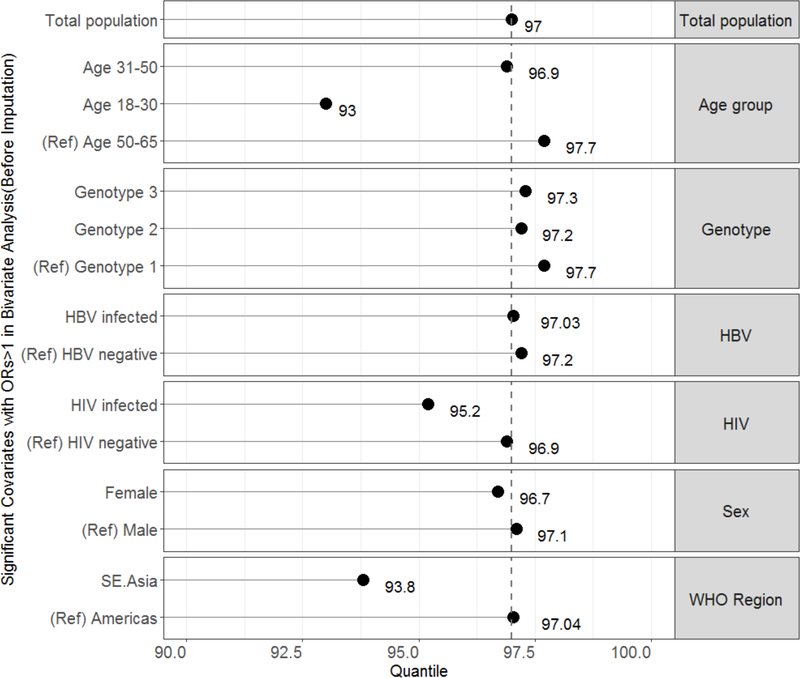
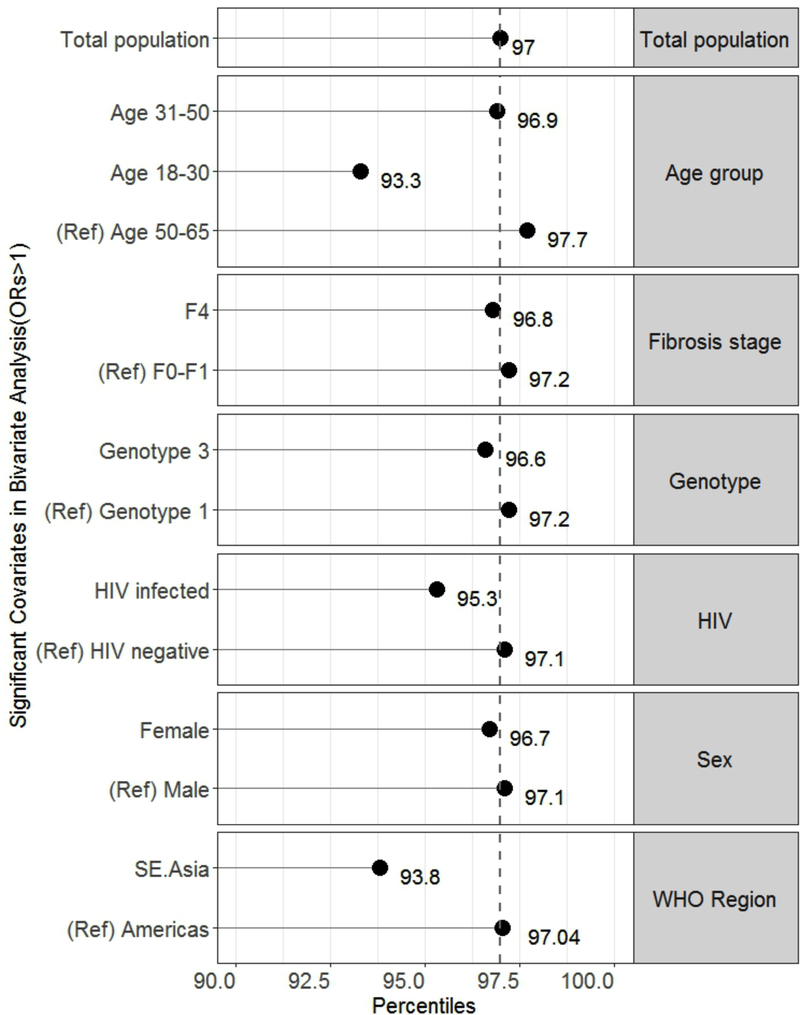
Methods: We established a multi-country cross-sectional dataset of first available quantitative HCV RNA measurements linked to demographic and clinical data. We excluded individuals on HCV treatment. We analysed the distribution of HCV RNA and determined critical thresholds for detection of HCV viraemia. We then performed logistic regression to evaluate factors associated with LLV, and derived relative sensitivities for significant covariates.
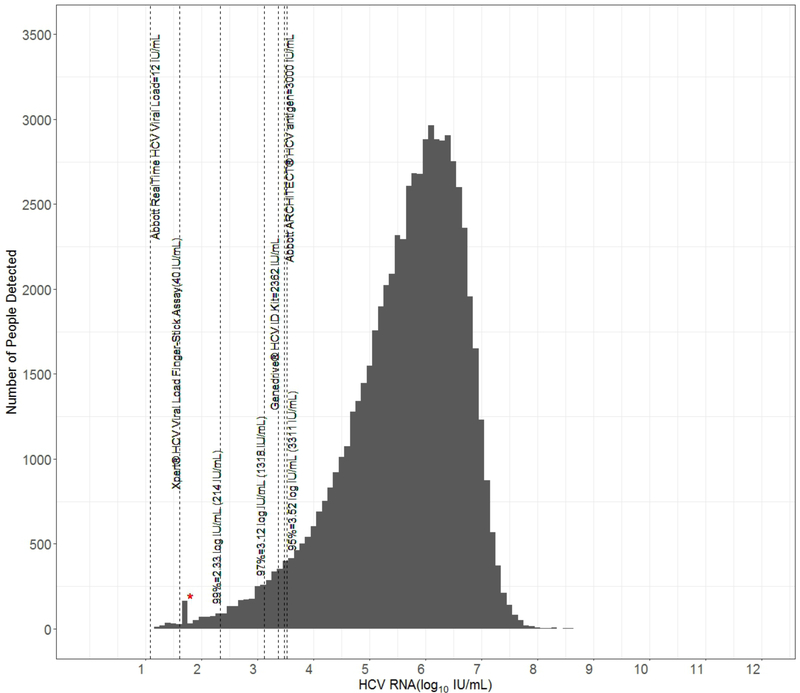
Results: The dataset included 66,640 individuals with HCV viraemia from across the world. The LOD for the 95th and 99th percentiles were 3,311 IU/ml and 214 IU/ml. The LOD for the 97th percentile was 1,318 IU/ml (95% CI 1,298.4-1,322.3). Factors associated with LLV, defined as HCV RNA <1,318 IU/ml, were younger age 18-30 vs. 51-64 years (odds ratios [OR] 2.56; 95% CI 2.19-2.99), female vs. male sex (OR 1.32; 95% CI 1.18-1.49), and advanced fibrosis stage F4 vs. F0-1 (OR 1.44; 95% CI 1.21-1.69). Only the younger age group had a decreased relative sensitivity below 95%, at 93.3%.
Conclusions: In this global dataset, a test with an LOD of 1,318 IU/ml would identify 97% of viraemic HCV infections among almost all populations. This LOD will help guide manufacturers in the development of affordable point-of-care diagnostics to expand HCV testing and linkage to care in low- and middle-income countries.
Lay summary: We created and analysed a dataset from 12 countries with 66,640 participants with chronic hepatitis C virus infection. We determined that about 97% of those with viraemic infection had 1,300 IU/ml or more of circulating virus at the time of diagnosis. While current diagnostic tests can detect as little as 12 IU/ml of virus, our findings suggest that increasing the level of detection closer to 1,300 IU/ml would maintain good test accuracy and will likely enable development of more affordable portable tests for use in low- and middle-income countries.
Keywords: Diagnosis; Hepatitis C virus; Limit of detection; Point-of-care; Viraemia, Affordable.
Copyright © 2019 European Association for the Study of the Liver. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Figures
References
-
- World Health Organization. Global Hepatitis Report 2017. 2017. [cited; Available from: http://www.who.int/hepatitis/publications/global-hepatitis-report2017/en/
-
- Global Tuberculosis Control Report Geneva; 2007.
-
- Gower E, Estes C, Blach S, Razavi-Shearer K, Razavi H. Global epidemiology and genotype distribution of the hepatitis C virus infection. J Hepatol 2014;61:S45–57. - PubMed
-
- World Health Organization. Global Health Sector Strategy on Viral Hepatitis 2016–2021: Towards Ending Hepatitis. 2016. [cited; Available from: http://www.who.int/hepatitis/strategy2016-2021/ghss-hep/en/
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
