

Effect of a HEART Care Pathway on Chest Pain Management Within an Integrated Health System
- PMID: 30797573
- PMCID: PMC6650318
- DOI: 10.1016/j.annemergmed.2019.01.007
Effect of a HEART Care Pathway on Chest Pain Management Within an Integrated Health System
Abstract
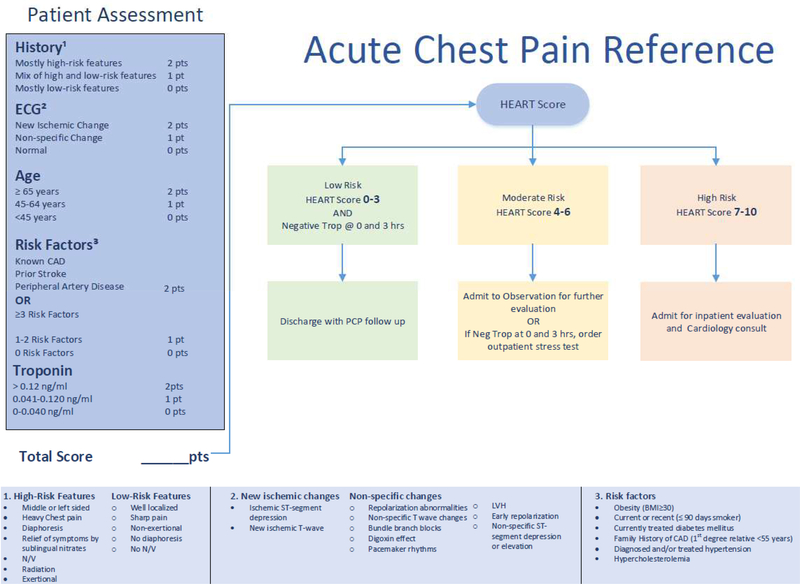
Study objective: We describe the association of implementing a History, ECG, Age, Risk Factors, and Troponin (HEART) care pathway on use of hospital care and noninvasive stress testing, as well as 30-day patient outcomes in community emergency departments (EDs).
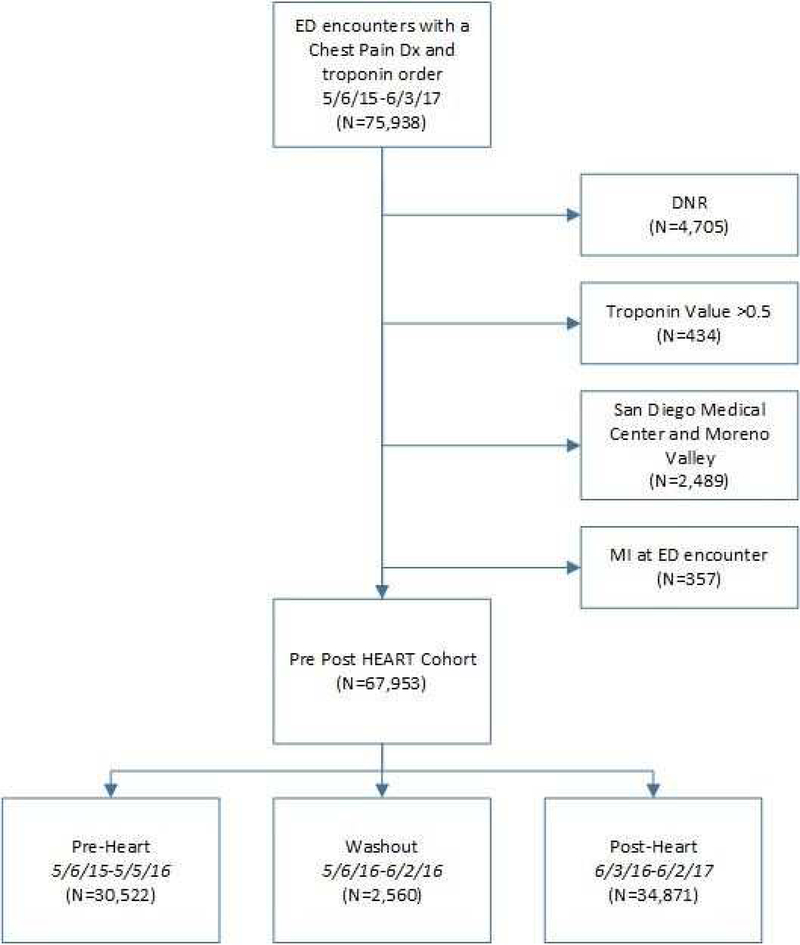
Methods: We performed a prospective interrupted-time-series study of adult encounters for patients evaluated for suspected acute coronary syndrome. The primary outcome was hospitalization or observation, noninvasive stress testing, or both within 30 days. The secondary outcome was 30-day all-cause mortality or acute myocardial infarction. A generalized estimating equation segmented logistic regression model was used to compare the odds of the primary outcome before and after HEART implementation. All models were adjusted for patient and facility characteristics and fit with physicians as a clustering variable.
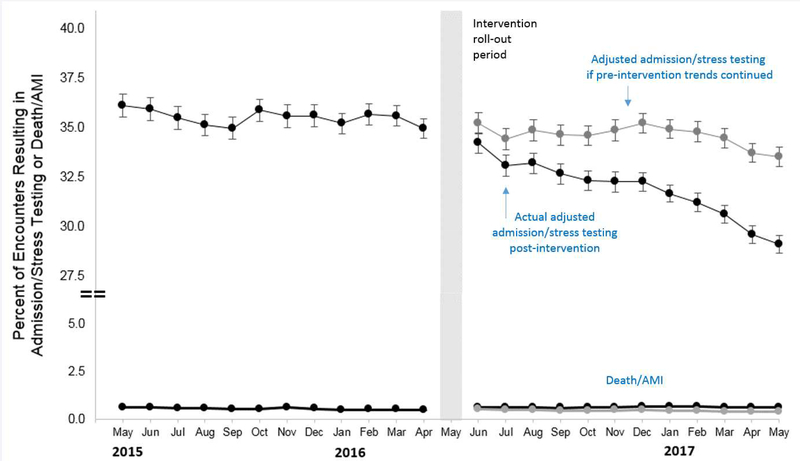
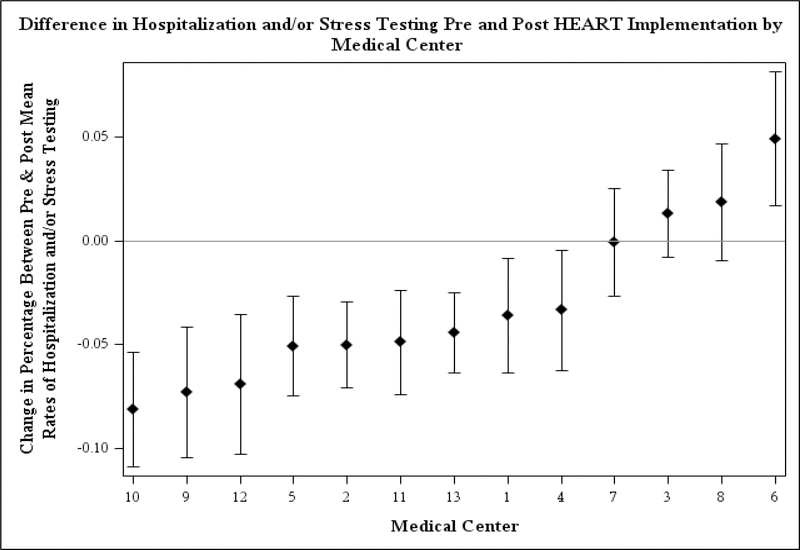
Results: A total of 65,393 ED encounters (before, 30,522; after, 34,871) were included in the study. Overall, 33.5% (before, 35.5%; after, 31.8%) of ED chest pain encounters resulted in hospitalization or observation, noninvasive stress testing, or both. Primary adjusted results found a significant decrease in the primary outcome postimplementation (odds ratio 0.984; 95% confidence interval [CI] 0.974 to 0.995). This resulted in an absolute adjusted month-to-month decrease of 4.39% (95% CI 3.72% to 5.07%) after 12 months' follow-up, with a continued trend downward. There was no difference in 30-day mortality or myocardial infarction (0.6% [before] versus 0.6% [after]; odds ratio 1.02; 95% CI 0.97 to 1.08).
Conclusion: Implementation of a HEART pathway in the ED evaluation of patients with chest pain resulted in less inpatient care and noninvasive cardiac testing and was safe. Using HEART to risk stratify chest pain patients can improve the efficiency and quality of care.
Copyright © 2019 American College of Emergency Physicians. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
Comment in
-
Can a HEART Pathway Improve Safety and Diagnostic Efficiency for Patients With Chest Pain?Ann Emerg Med. 2019 Aug;74(2):181-184. doi: 10.1016/j.annemergmed.2019.02.030. Epub 2019 May 9. Ann Emerg Med. 2019. PMID: 31080033 No abstract available.
References
-
- Prevention CfDCa. National Hospital Ambulatory Medical Care Survey: 2010 Emergency Department Summary Tables. 2010.
-
- Sabbatini AK, Nallamothu BK, Kocher KE. Reducing variation in hospital admissions from the emergency department for low-mortality conditions may produce savings. Health Aff (Millwood). 2014;33(9):1655–1663. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
