

Kinesiologic considerations for targeting activation of scapulothoracic muscles - part 2: trapezius
- PMID: 30797676
- PMCID: PMC6849087
- DOI: 10.1016/j.bjpt.2019.01.011
Kinesiologic considerations for targeting activation of scapulothoracic muscles - part 2: trapezius
Abstract
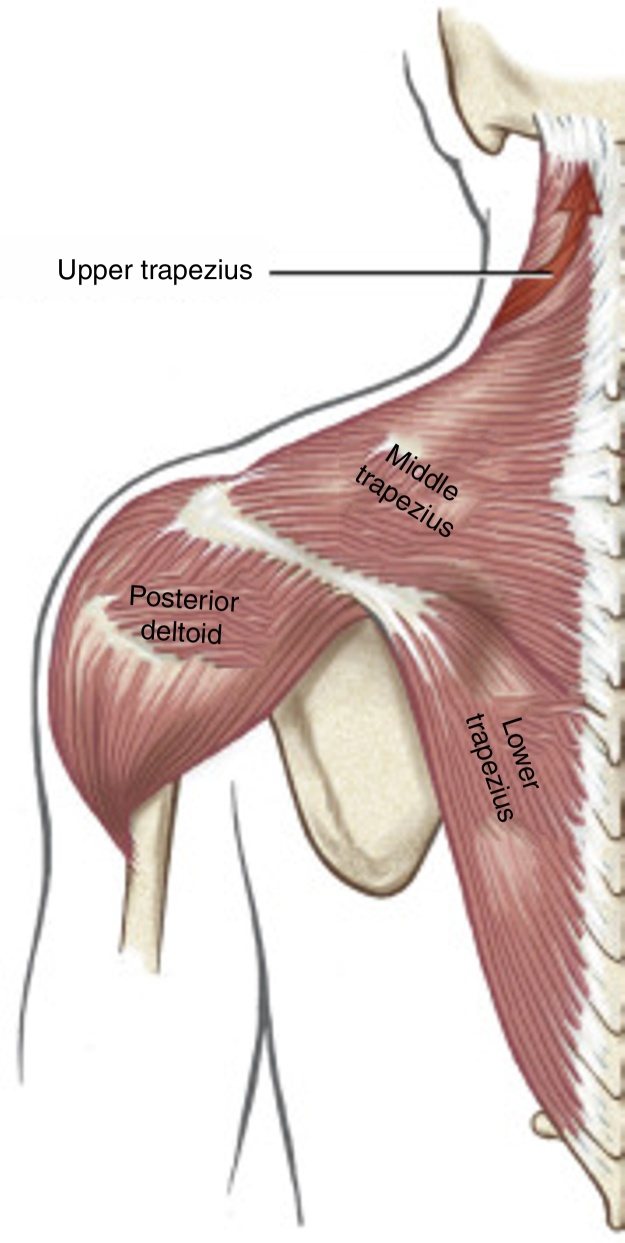
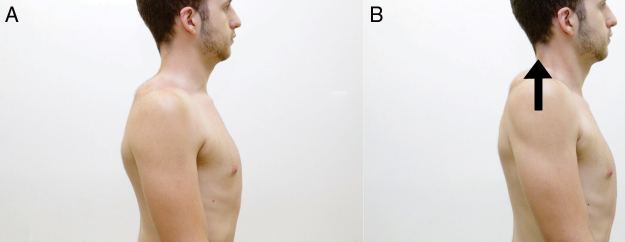
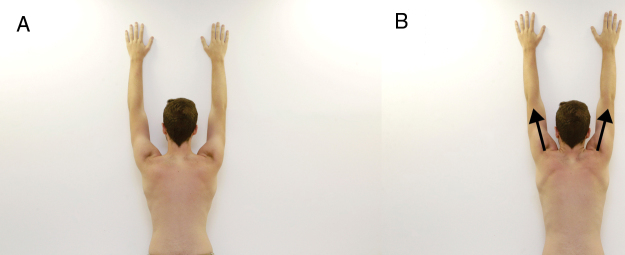
Background: The trapezius is an extensive muscle subdivided into upper, middle, and lower parts. This muscle is a dominant stabilizer of the scapula, normally operating synergistically with other scapular muscles, most notably the serratus anterior. Altered activation, poor control, or reduced strength of the different parts of the trapezius have been linked with abnormal scapular movements, often associated with pain. Several exercises have been designed and studied that specifically target the different parts of the trapezius, with the goal of developing exercises that optimize scapular position and scapulohumeral rhythm that reduce pain and increase function.
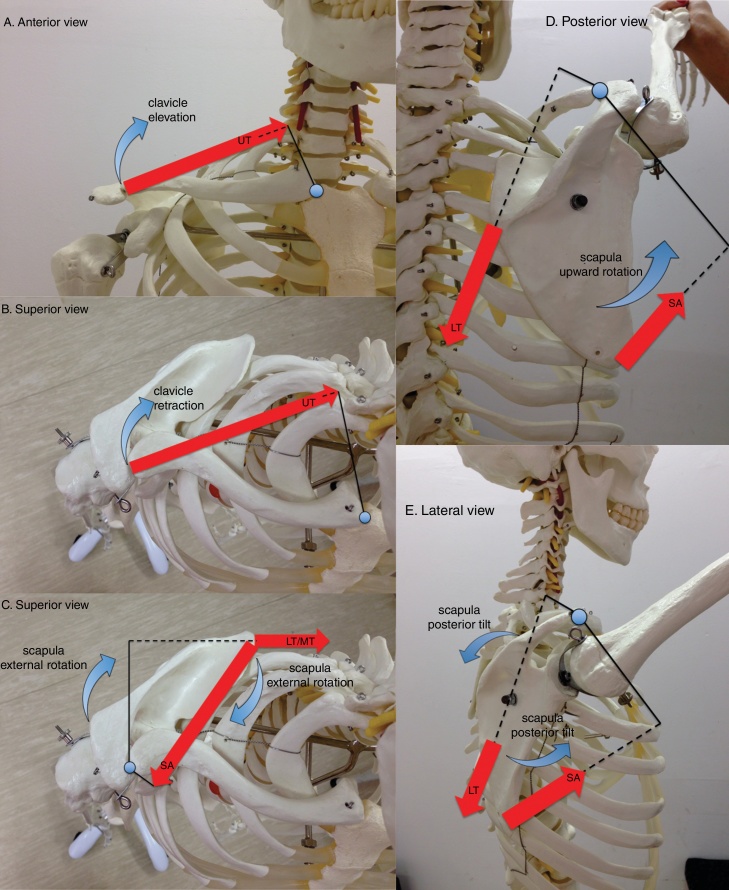
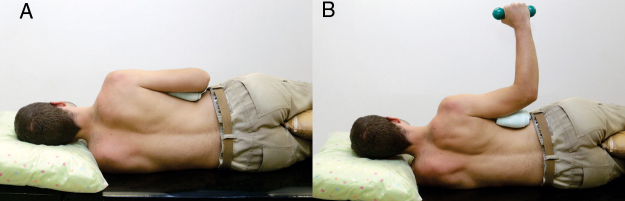
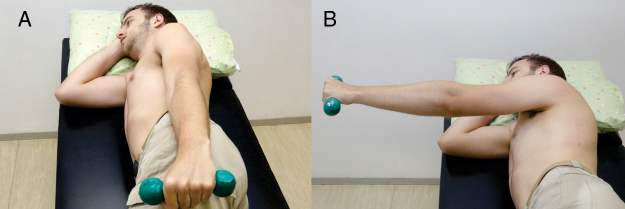
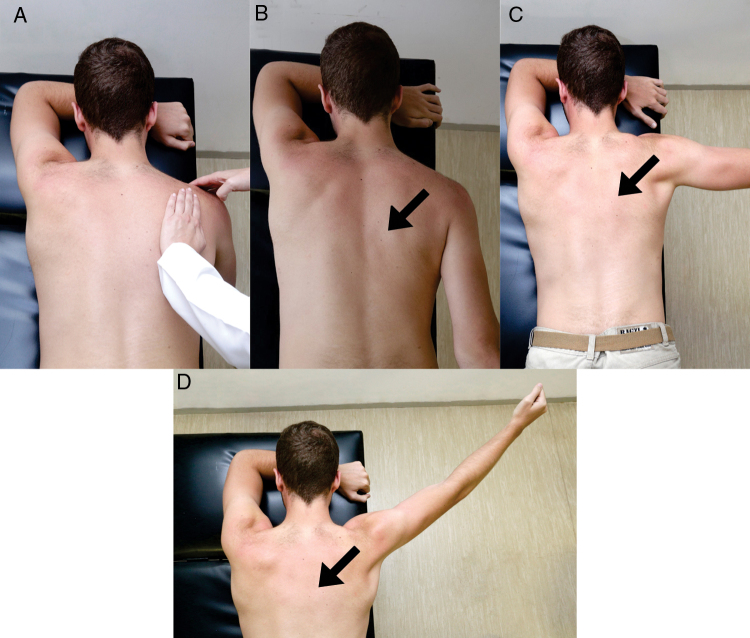
Methods: This paper describes the anatomy, kinesiology, and pathokinesiology of the trapezius as well as exercises that selectively target the activation of the different parts of this complex muscle.
Conclusions: This review provides the anatomy and kinesiology of the trapezius muscle with the underlying intention of understanding how this muscle contributes to the normal mechanics of the scapula as well as the entire shoulder region. This paper can guide the clinician with planning exercises that specifically target the different parts of the trapezius. It is recommended that this paper be read as a companion to another paper: Kinesiologic considerations for targeting activation of scapulothoracic muscles - part 1: serratus anterior.
Keywords: Physical therapy; Scapular dyskinesis; Scapulothoracic joint; Shoulder rehabilitation; Trapezius exercises.
Copyright © 2019 Associação Brasileira de Pesquisa e Pós-Graduação em Fisioterapia. Publicado por Elsevier Editora Ltda. All rights reserved.
Figures


References
-
- De Vita A., Kibler W.B., Pouliart N., Sciascia A. Scapulothoracic joint. In: Di Giacomo G., Pouliart N., Constantini A., DeVita A., editors. Atlas of Functional Shoulder Anatomy. 1st ed. Springer; Milan: 2008.
-
- Wiater J.M., Bigliani L.U. Spinal accessory nerve injury. Clin Orthop Relat Res. 1999;(368):5–16. - PubMed
-
- Chan P.K., Hems T.E. Clinical signs of accessory nerve palsy. J Trauma. 2006;60(5):1142–1144. - PubMed
-
- Neumann D.A. 3rd ed. Elsevier; St Louis: 2017. Kinesiology of the Musculoskeletal System: Foundations for Rehabilitation.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
