

Estimates of case-fatality ratios of measles in low-income and middle-income countries: a systematic review and modelling analysis
- PMID: 30797735
- PMCID: PMC6418190
- DOI: 10.1016/S2214-109X(18)30537-0
Estimates of case-fatality ratios of measles in low-income and middle-income countries: a systematic review and modelling analysis
Abstract
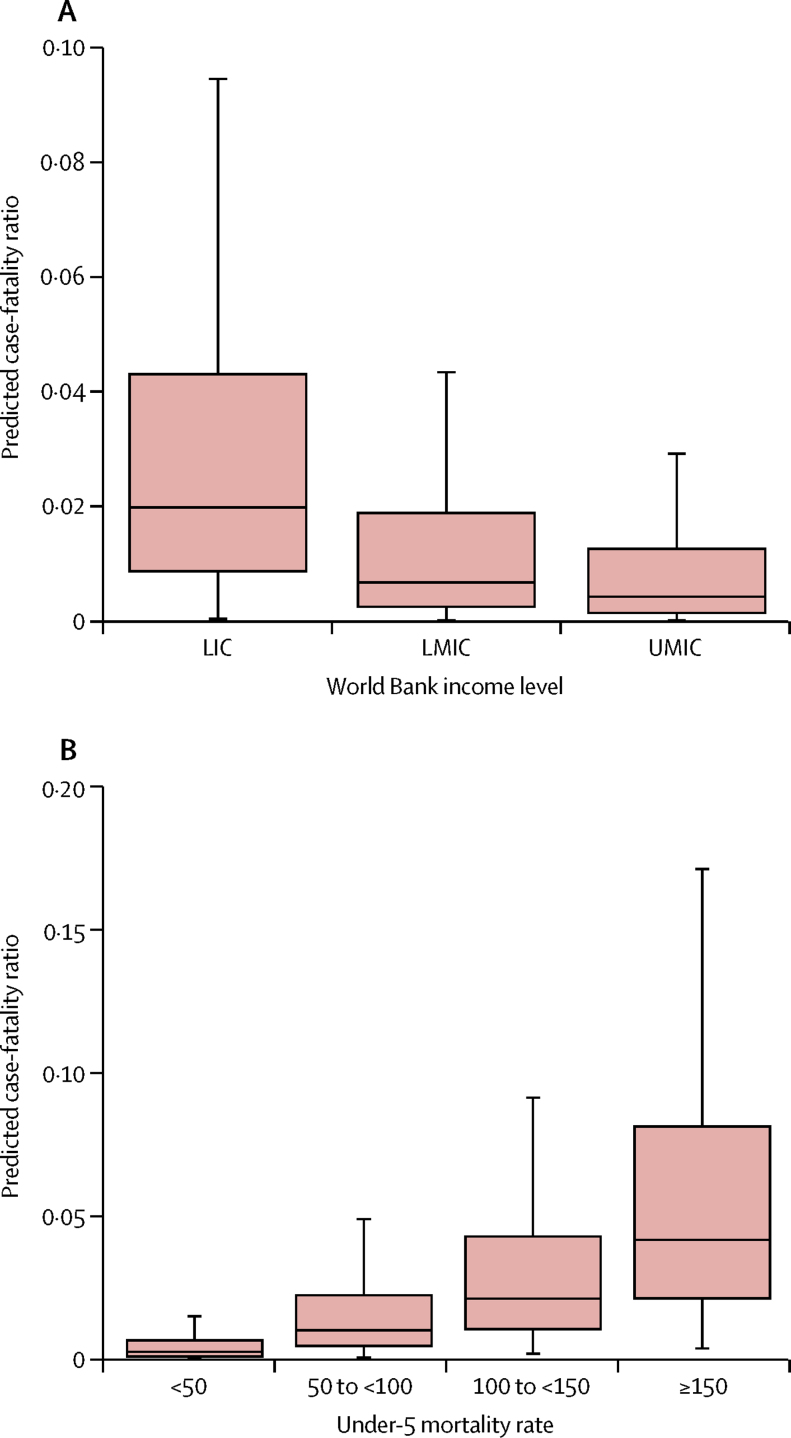
Background: In the 21st century, increases in immunisation coverage and decreases in under-5 mortality have substantially reduced the global burden of measles mortality. However, the assessment of measles mortality burden is highly dependent on estimates of case-fatality ratios for measles, which can vary according to geography, health systems infrastructure, prevalence of underlying risk factors, and measles endemicity. With imprecise case-fatality ratios, there is continued uncertainty about the burden of measles mortality and the effect of measles vaccination. In this study, we aimed to update the estimations of case-fatality ratios for measles, to develop a prediction model to estimate case-fatality ratios across heterogeneous groupings, and to project future case-fatality ratios for measles up to 2030.
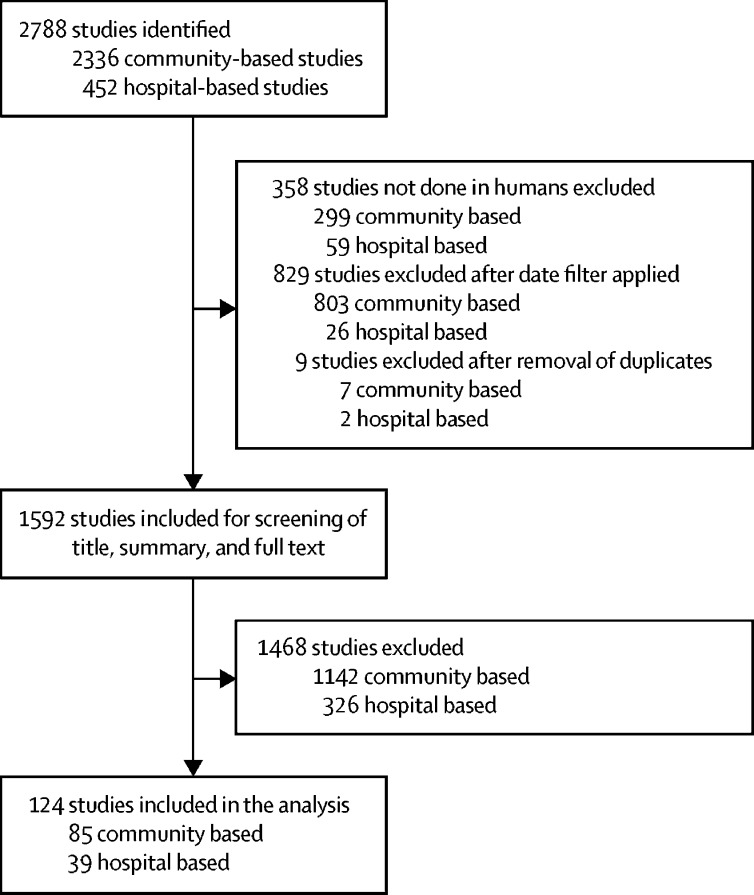
Methods: We did a review of the literature to identify studies examining measles cases and deaths in low-income and middle-income countries in all age groups from 1980 to 2016. We extracted data on case-fatality ratios for measles overall and by age, where possible. We developed and examined several types of generalised linear models and determined the best-fit model according to the Akaike information criterion. We then selected a best-fit model to estimate measles case-fatality ratios from 1990 to 2015 and projected future case-fatality ratios for measles up to 2030.
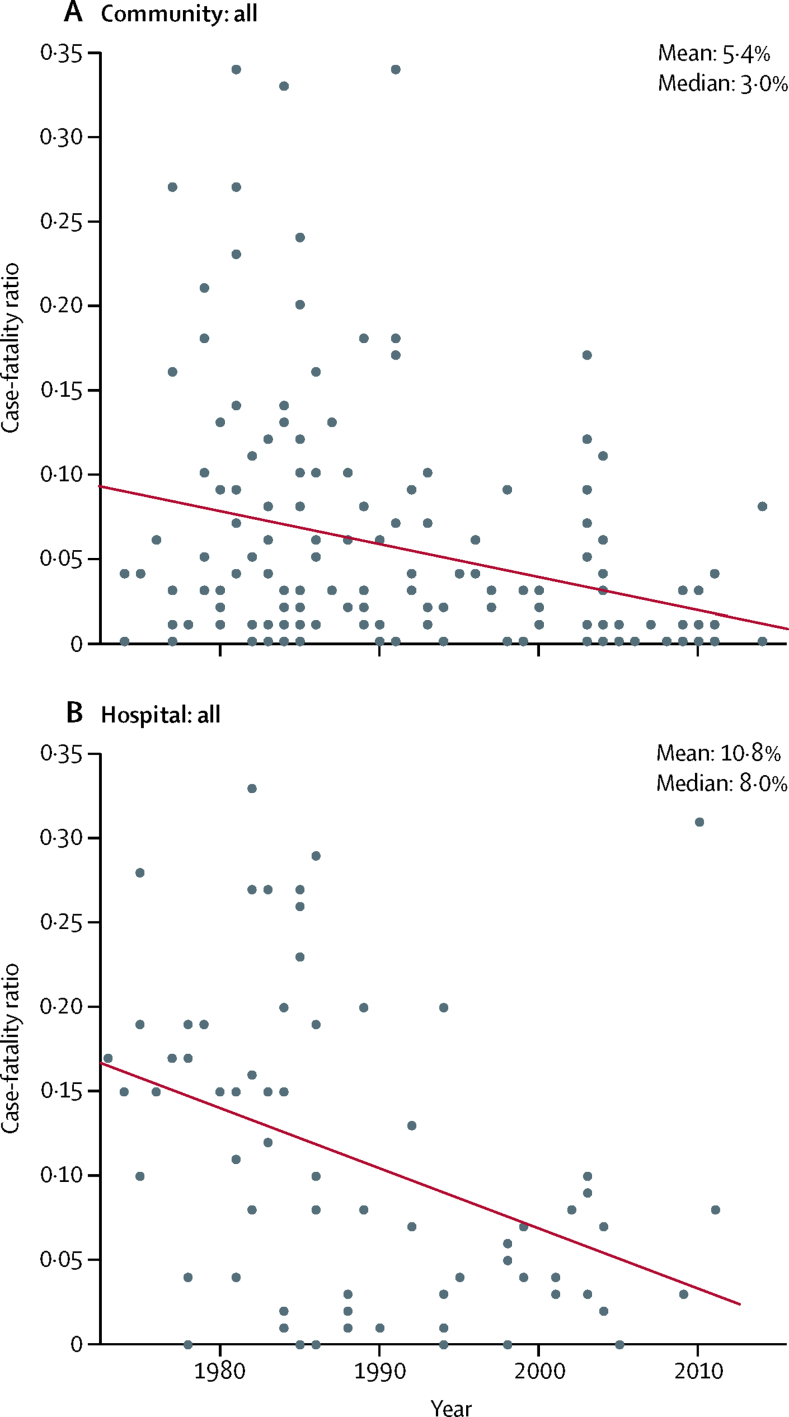
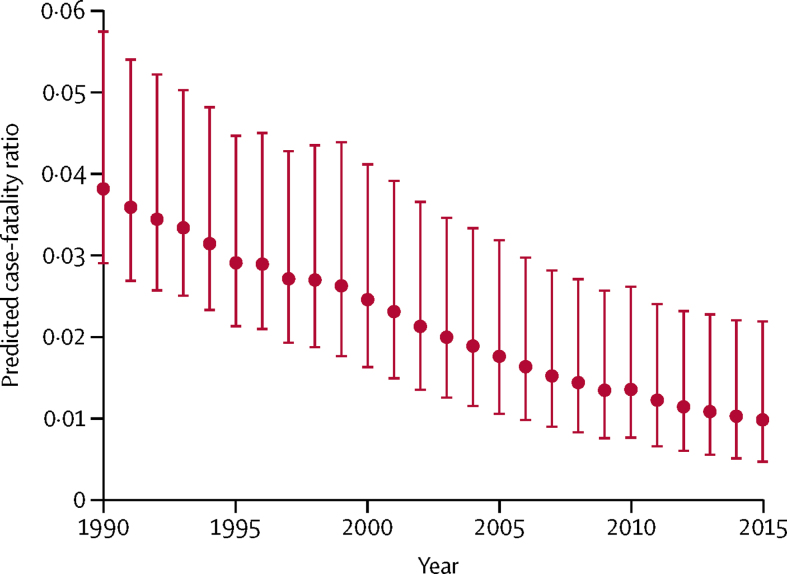
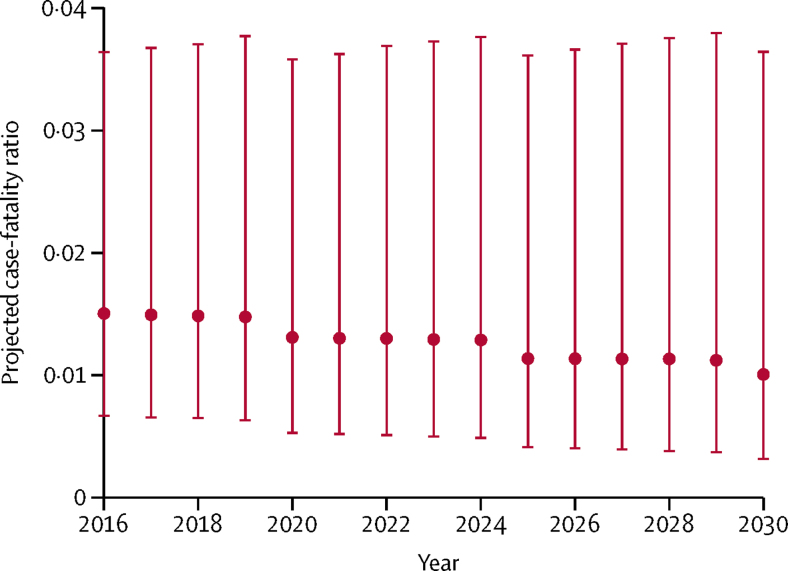
Findings: We selected 124 peer-reviewed journal articles published between Jan 1, 1980, and Dec 31, 2016, for inclusion in the final review-85 community-based studies and 39 hospital-based studies. We selected a log-linear prediction model, resulting in a mean case-fatality ratio of 2·2% (95% CI 0·7-4·5) in 1990-2015. In community-based settings, the mean case-fatality ratio was 1·5% (0·5-3·1) compared with 2·9% (0·9-6·0) in hospital-based settings. The mean projected case-fatality ratio in 2016-2030 was 1·3% (0·4-3·7).
Interpretation: Case-fatality ratios for measles have seen substantial declines since the 1990s. Our study provides an updated estimation of case-fatality ratios that could help to refine assessment of the effect on mortality of measles control and elimination programmes.
Funding: Bill & Melinda Gates Foundation.
Copyright © 2019 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
What will it take to end fatalities from measles?Lancet Glob Health. 2019 Apr;7(4):e394-e395. doi: 10.1016/S2214-109X(19)30050-6. Epub 2019 Feb 21. Lancet Glob Health. 2019. PMID: 30797736 No abstract available.
References
-
- Simons E, Ferrari M, Fricks J. Assessment of the 2010 global measles mortality reduction goal: results from a model of surveillance data. Lancet. 2012;379:2173–2178. - PubMed
-
- Samb B, Aaby P, Whittle H, Seck AM, Simondon F. Decline in measles case fatality ratio after the introduction of measles immunization in rural Senegal. Am J Epidemiol. 1997;145:51–57. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
