

Magnetic resonance imaging spectrum of intracranial tubercular lesions: one disease, many faces
- PMID: 30800191
- PMCID: PMC6384409
- DOI: 10.5114/pjr.2018.81408
Magnetic resonance imaging spectrum of intracranial tubercular lesions: one disease, many faces
Abstract
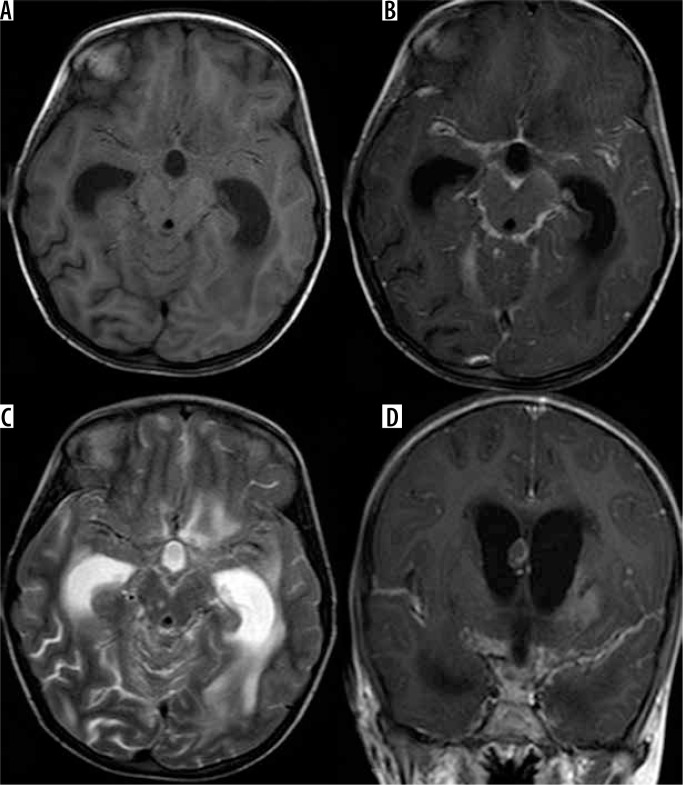
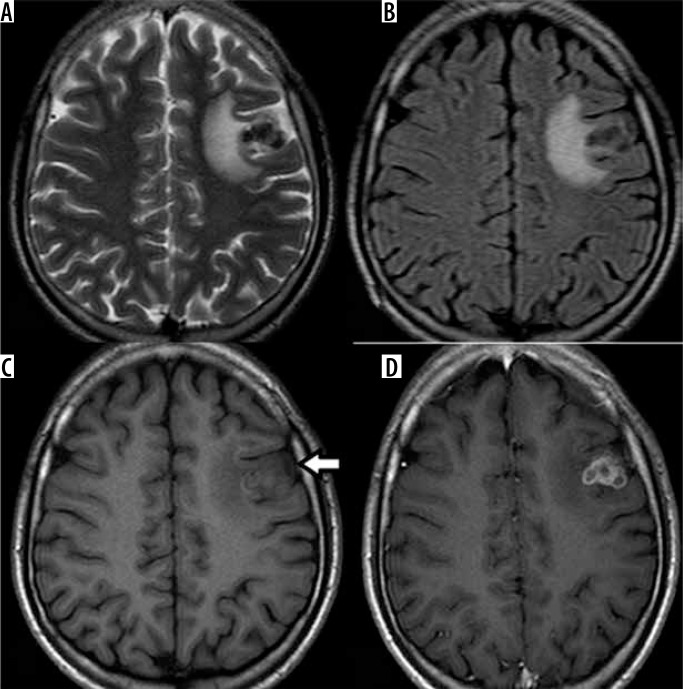
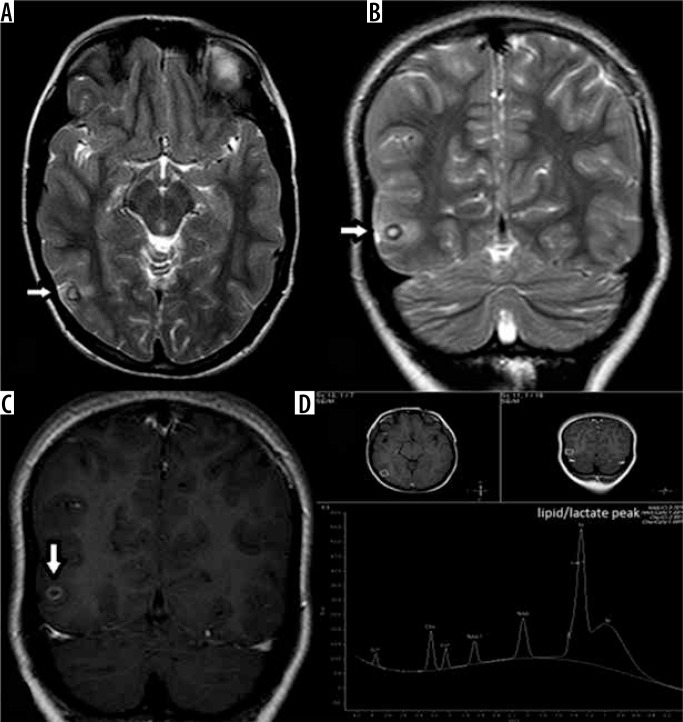
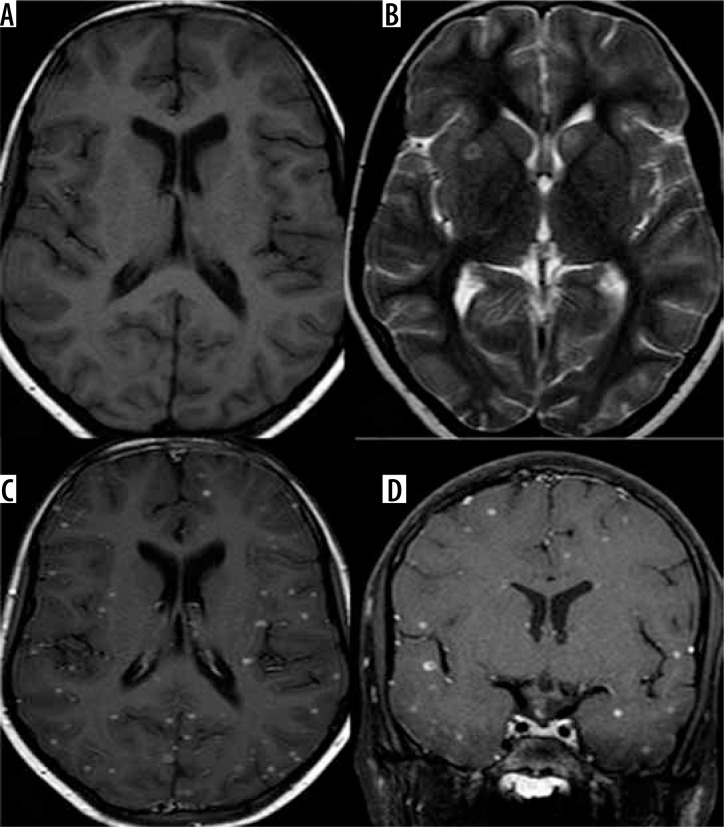
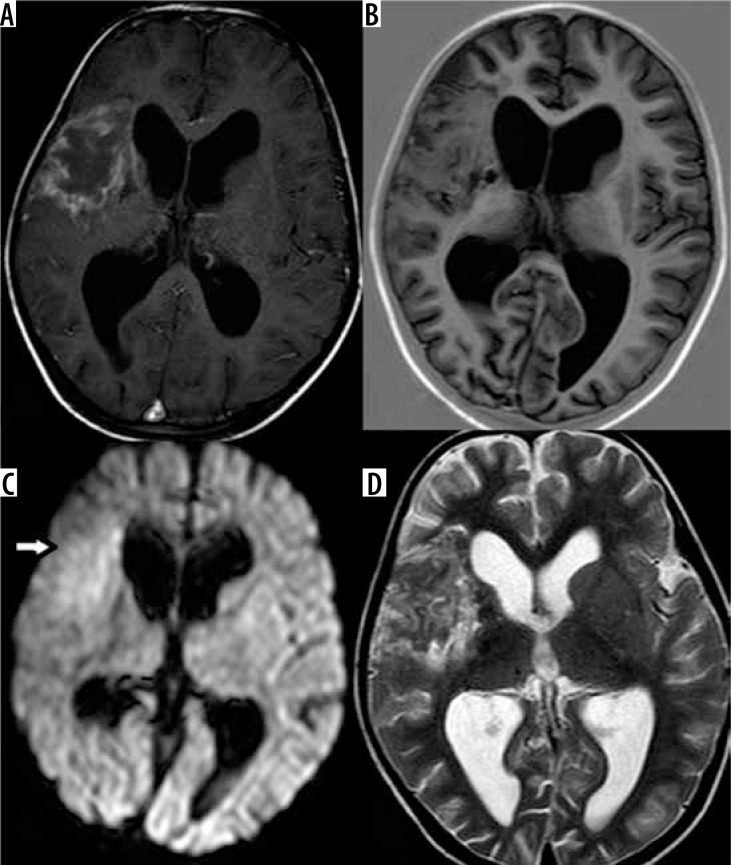
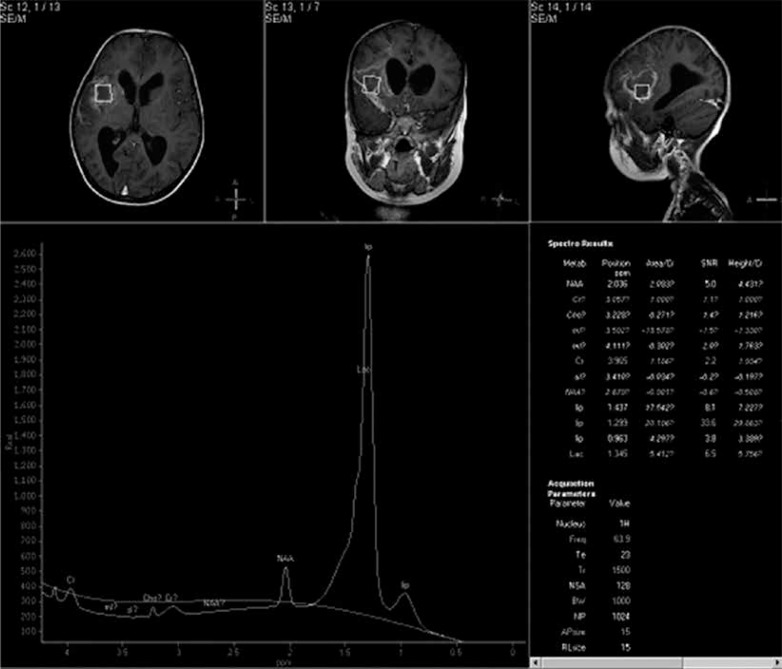
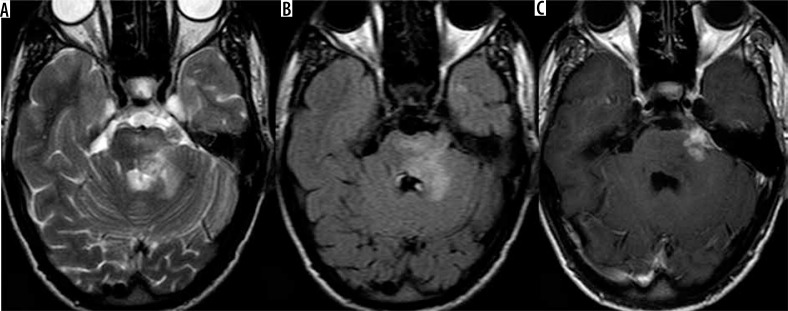
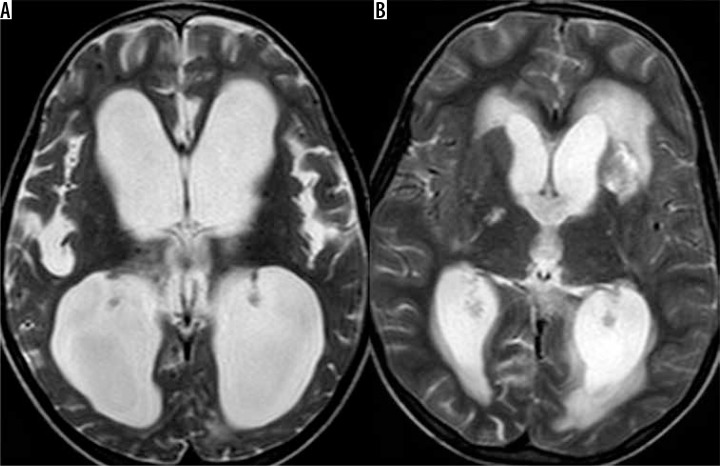
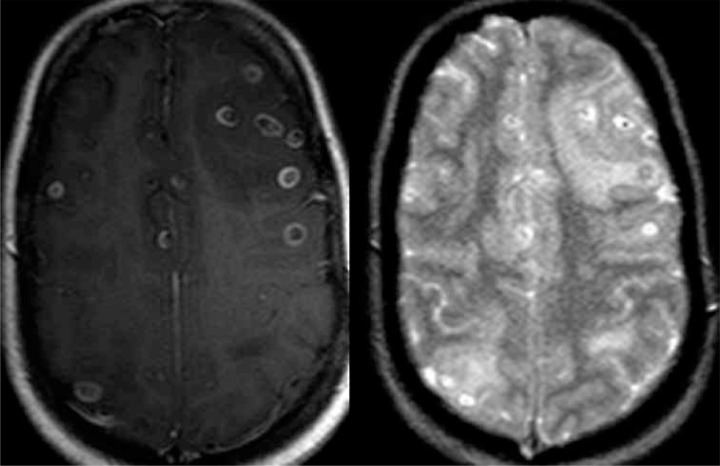
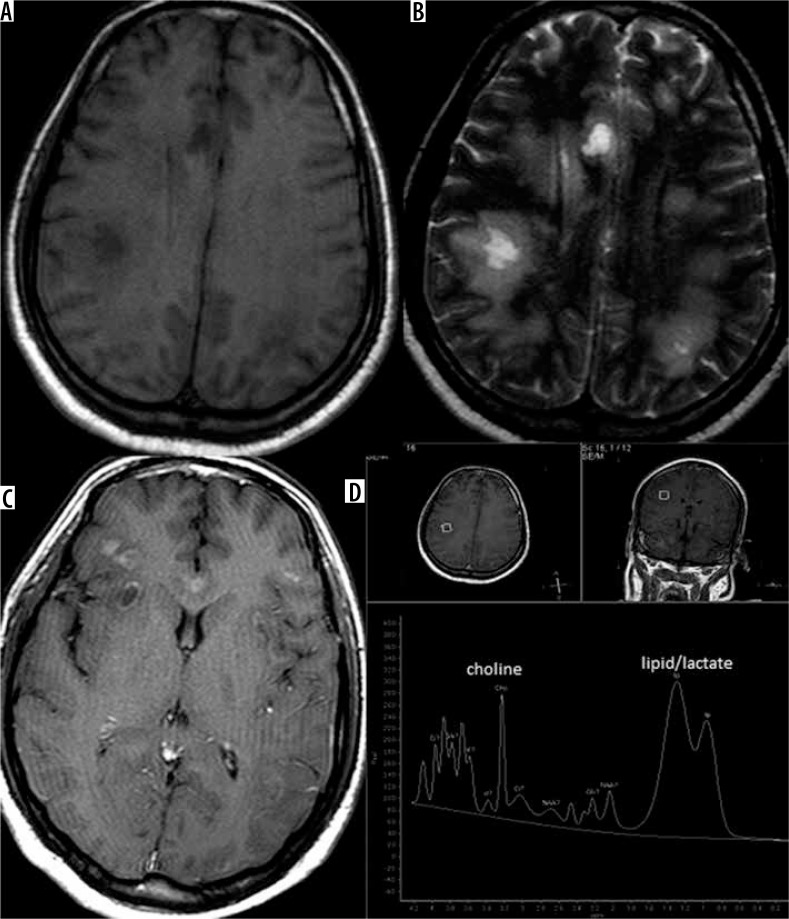
Tuberculosis is a devastating disease and has shown resurgence in recent years with the advent of acquired immunodeficiency syndrome. Central nervous system involvement is the most devastating form of the disease, comprising 10% of all tuberculosis cases. The causative organism, Mycobacterium tuberculosis, incites a granulomatous inflammatory response in the brain, the effects of which can be appreciated on magnetic resonance imaging (MRI), which can thus be used for diagnosis of the same. Neurotuberculosis can present in various patterns, which can be identified on MRI. The meningeal forms include leptomeningitis and pachymeningitis. Parenchymal forms of neurotuberculosis include tuberculoma in its various stages, tubercular cerebritis and abscess, tubercular rhombencephalitis, and tubercular encephalopathy. Each pattern has characteristic MRI appearances and differential diagnoses on imaging. Complications of neurotuberculosis, usually of tubercular meningitis, include hydrocephalus, vasculitis, and infarcts as well as cranial nerve palsies. Various MRI sequences besides the conventional ones can provide additional insight into the disease, help in quantifying the disease load, and help in differentiation of neurotuberculosis from conditions with similar imaging appearances and presentations. These can enable accurate and timely diagnosis by the radiologist and early institution of treatment in order to reduce the likelihood of permanent neurological sequelae.
Keywords: MRI; brain; spectroscopy; tuberculoma; tuberculosis.
Conflict of interest statement
The authors report no conflict of interest.
Figures
References
-
- Torres C, Riascos R, Figueroa R, Gupta RK. Central nervous system tuberculosis. Top Magn Reson Imaging. 2014;23:173–189. - PubMed
-
- Bernaerts A, Vanhoenacker FM, Parizel PM, et al. Tuberculosis of the central nervous system: overview of neuroradiological findings. Eur Radiol. 2003;13:1876–1890. - PubMed
-
- Vidal JE, de Oliveira AC, Filho FB, et al. Tuberculous brain abscess in AIDS patients: report of three cases and literature review. Int J Infect Dis. 2005;9:201–207. - PubMed
Publication types
LinkOut - more resources
Full Text Sources