

Tumefactive Multiple Sclerosis, A Rare Variant Presenting as Multiple Ring-enhancing Lesions in an Immunocompetent Patient: A Case Report
- PMID: 30800548
- PMCID: PMC6384036
- DOI: 10.7759/cureus.3738
Tumefactive Multiple Sclerosis, A Rare Variant Presenting as Multiple Ring-enhancing Lesions in an Immunocompetent Patient: A Case Report
Abstract
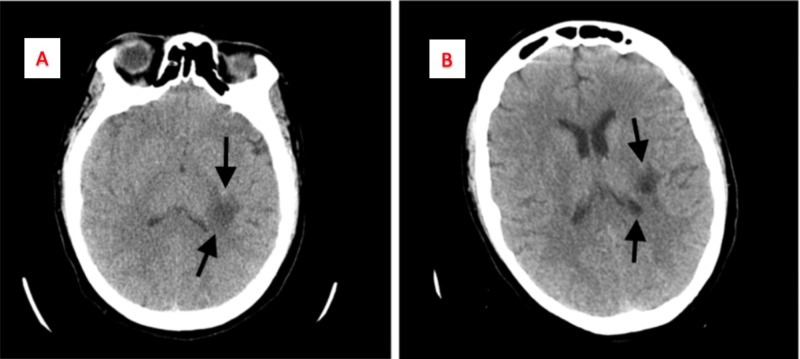
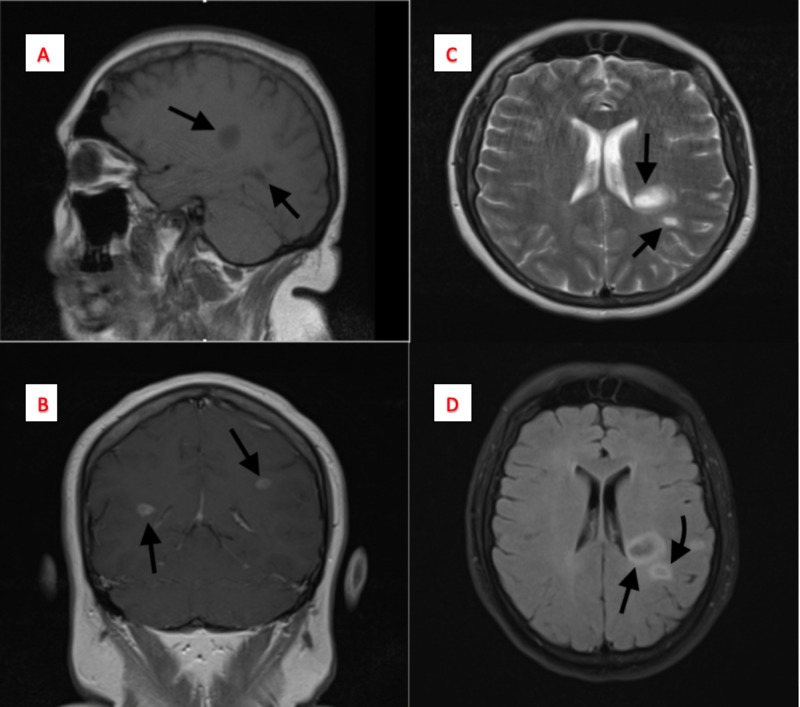
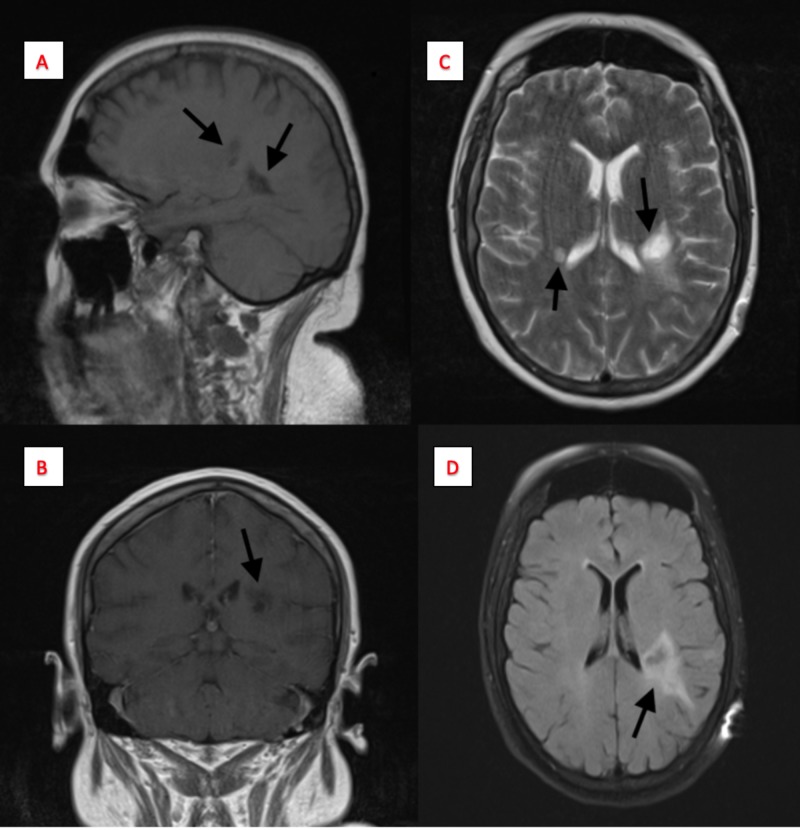
Tumefactive multiple sclerosis (TMS) is a rare entity which can be difficult to diagnose unless definitive diagnostic measures are taken. TMS is characterized by solitary or multiple lesions that are sized > 2 cm, with/without mass effect, edema, and ring enhancement on magnetic resonance imaging (MRI). The demyelinating lesion can mimic infections, vascular lesions, and inflammatory lesions. The clinical presentation is highly dependent on the area of the brain which is affected, and this can lead to a variety of signs and symptoms. Herein, we present the case of a 40-year-old immunocompetent female with a history of right-sided numbness of her face, arm, and leg associated with muscle weakness for about a week. Workup included an MRI showing ring-enhancing lesions in the white matter of the brain, zero oligoclonal bands in the CSF, a normal immunoglobulin G (IgG) index, and an elevated myelin basic protein (MBP) in the CSF. A biopsy was obtained that showed predominant macrophage infiltrate with loss of myelin but the preservation of axons. Suspecting a demyelinating pathology, the patient was informed that she would be started on intravenous dexamethasone for an eight-day course. With subsequent completion of this course in the hospital, the patient was discharged on oral prednisone daily for a month and a referral leading to a definitive diagnosis of TMS. The patient was started on interferon beta-1a and subsequently relapsed due to noncompliance. However, further workup showed a reduction in the mass-like lesions and a response to therapy. If suspicion for TMS is high despite workup, steroids can be used with immunomodulators in the interim to combat symptoms and potentially reduce lesions and potentially subvert the need for biopsy.
Keywords: immunocompetent; immunomodulators; ms therapy; multiple sclerosis; ring-enhancing lesion; space-occupying lesion; tms therapy; tumefactive multiple sclerosis (tms).
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Unusual Stroke-Like Presentation of Tumefactive Multiple Sclerosis in a 27-Year-Old Man.Cureus. 2025 Mar 2;17(3):e79909. doi: 10.7759/cureus.79909. eCollection 2025 Mar. Cureus. 2025. PMID: 40171340 Free PMC article.
-
Tumefactive multiple sclerosis (TMS): A case series of this challenging variant of MS.Mult Scler Relat Disord. 2021 Feb;48:102699. doi: 10.1016/j.msard.2020.102699. Epub 2020 Dec 26. Mult Scler Relat Disord. 2021. PMID: 33373797
-
Diagnostic Challenges and Radiological Spectrum of Tumefactive Multiple Sclerosis: A Case Report Study.Cureus. 2022 Nov 26;14(11):e31899. doi: 10.7759/cureus.31899. eCollection 2022 Nov. Cureus. 2022. PMID: 36579264 Free PMC article.
-
A challenging diagnosis of late-onset tumefactive multiple sclerosis associated to cervicodorsal syringomyelia: doubtful CT, MRI, and bioptic findings: Case report and literature review.Medicine (Baltimore). 2016 Sep;95(36):e4585. doi: 10.1097/MD.0000000000004585. Medicine (Baltimore). 2016. PMID: 27603348 Free PMC article. Review.
-
Tumefactive demyelinating lesions: A comprehensive review.Mult Scler Relat Disord. 2017 May;14:72-79. doi: 10.1016/j.msard.2017.04.003. Epub 2017 Apr 9. Mult Scler Relat Disord. 2017. PMID: 28619436 Review.
Cited by
-
Tumefactive Multiple Sclerosis of the Cervical Spinal Cord: A Rare Case Report.Cureus. 2020 Jan 23;12(1):e6754. doi: 10.7759/cureus.6754. Cureus. 2020. PMID: 32140322 Free PMC article.
-
Long-term outcomes of ADEM-like and tumefactive presentations of CNS demyelination: a case-comparison analysis.J Neurol. 2024 Aug;271(8):5275-5289. doi: 10.1007/s00415-024-12349-6. Epub 2024 Jun 11. J Neurol. 2024. PMID: 38861035 Free PMC article.
References
-
- It is not a tumor: a rare case of tumefactive multiple sclerosis. Smith C, Finan M, Axelband J, Williams K. Am J Emerg Med. 2014;32:946–943. - PubMed
-
- Tumefactive demyelination: an approach to diagnosis and management. Hardy TA, Chataway J. J Neurol Neurosurg Psychiatry. 2013;84:1047–1053. - PubMed
-
- Distinguishing tumefactive demyelinating lesions from glioma or central nervous system lymphoma: added value of unenhanced CT compared with conventional contrast-enhanced MR imaging. Kim DS, Na DG, Kim KH, Kim JH, Kim E, Yun B La, Chang KH. Radiology. 2009;251:467–475. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous