

Performance of a 2-step insulin infusion protocol with adjustment of insulin doses for Asians in the medical intensive care unit following cardiothoracic surgery
- PMID: 30800560
- PMCID: PMC6357233
- DOI: 10.1007/s13340-018-0358-y
Performance of a 2-step insulin infusion protocol with adjustment of insulin doses for Asians in the medical intensive care unit following cardiothoracic surgery
Abstract
Background: Most previous insulin infusion protocols are titrated for Westerners and are not simple to follow. In this study, we tested the efficacy and safety of our simple insulin infusion protocol utilizing lower insulin doses for Asians.
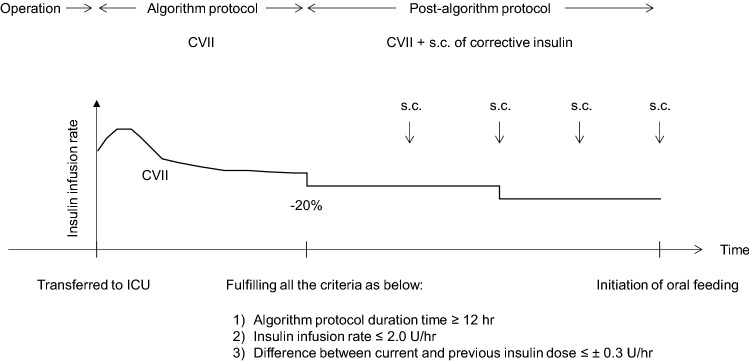
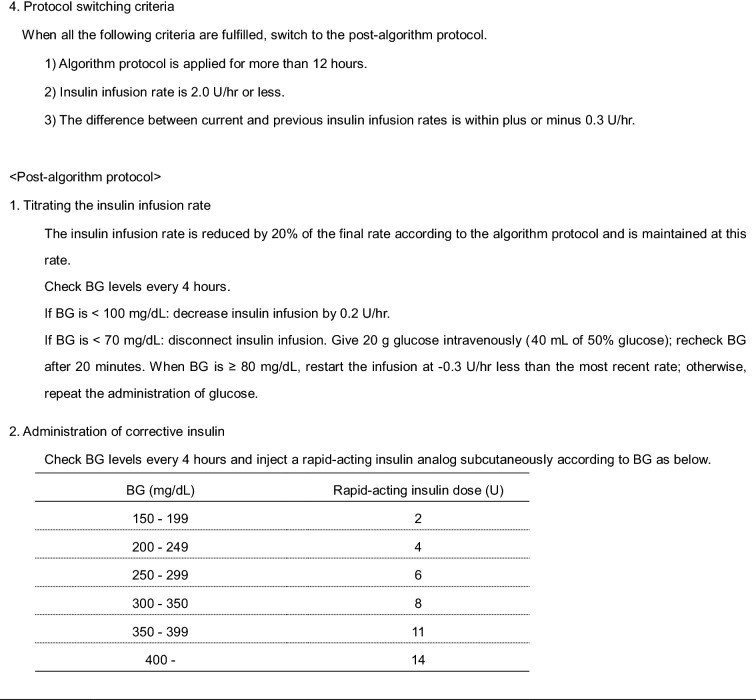
Methods: A total of 152 patients with type 2 diabetes undergoing cardiothoracic surgery were included. After surgery, blood glucose (BG) was initially managed according to our algorithm protocol, and subsequently by the post-algorithm protocol. Insulin infusion rates in the algorithm protocol were titrated in two steps according to (1) current BG levels and (2) the difference between current and previous BG levels. In the post-algorithm protocol, insulin lispro was injected subcutaneously in addition to intravenous insulin infusion according to BG levels. The efficacy was assessed as achievement rates of two target BG ranges (140-199 and 80-199 mg/dL), and safety was assessed as hypoglycemia (< 70 mg/dL) and protocol error rates.
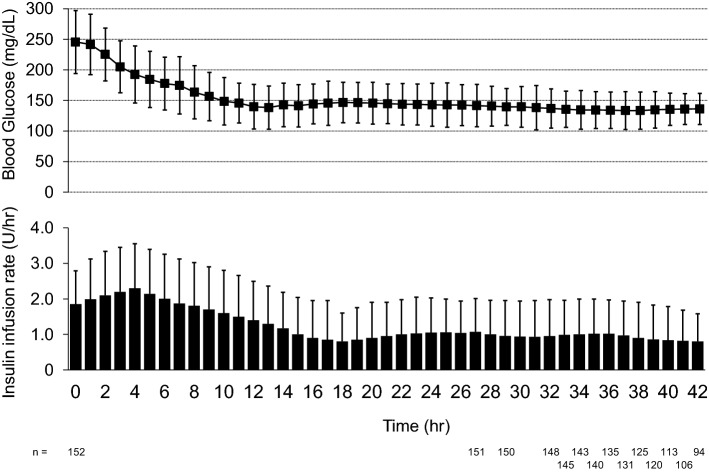
Results: With the use of the algorithm protocol, 58.7% of 1749 BG measurements achieved a range of 140-199 mg/dL, and 95.9% achieved levels within the 80-199 mg/dL range. Hypoglycemia and protocol error rates were 0.47 and 0.51%, respectively. With the post-algorithm protocol, 48.7 and 98.3% of 898 BG measurements achieved each target range. Hypoglycemia and protocol error rates were 0.78 and 0.22%, respectively. Severe hypoglycemia (< 40 mg/dL) was not observed.
Conclusions: Our insulin infusion protocol seems to be efficacious, safe, and widely feasible for Asian patients because of its simplicity and lower insulin dose.
Keywords: Cardiac surgery; Hypoglycemia; Insulin; Insulin infusion protocol; Intensive care unit; Surgical diabetes.
Conflict of interest statement
All the authors declare that they have no conflict of interest.Yoshihiko Nishio has received honoraria for scientific lectures from Eli Lilly. Kazuma Ogiso, Nobuyuki Koriyama, Takahiko Obo, Akinori Tokito, and Takayuki Ueno have nothing to disclose.All the procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (National Hospital Organization Kagoshima Medical Center, Ethics Committee, date of approval: 6 February 2017, approval no. 28-71) and with the Helsinki Declaration of 1964 and later versions.
Figures



Similar articles
-
Performance of a dose-defining insulin infusion protocol among trauma service intensive care unit admissions.Diabetes Technol Ther. 2006 Aug;8(4):476-88. doi: 10.1089/dia.2006.8.476. Diabetes Technol Ther. 2006. PMID: 16939372
-
Evaluation of nursing adherence to a paper-based graduated continuous intravenous regular human insulin infusion algorithm.Nutrition. 2012 Oct;28(10):1008-11. doi: 10.1016/j.nut.2012.01.010. Epub 2012 May 31. Nutrition. 2012. PMID: 22658642
-
A unified Hyperglycemia and Diabetic ketoacidosis (DKA) insulin infusion protocol based on an Excel algorithm and implemented via Electronic Medical Record (EMR) in Intensive Care Units.Diabetes Metab Syndr. 2017 Oct-Dec;11(4):265-271. doi: 10.1016/j.dsx.2016.09.008. Epub 2016 Sep 15. Diabetes Metab Syndr. 2017. PMID: 27658894
-
Perioperative control of blood glucose level in cardiac surgery.Gen Thorac Cardiovasc Surg. 2013 Feb;61(2):61-6. doi: 10.1007/s11748-012-0198-9. Epub 2013 Jan 5. Gen Thorac Cardiovasc Surg. 2013. PMID: 23292688 Review.
-
Algorithms for intravenous insulin delivery.Curr Diabetes Rev. 2008 Aug;4(3):258-68. doi: 10.2174/157339908785294451. Curr Diabetes Rev. 2008. PMID: 18690908 Review.
Cited by
-
Protective role of Tongxinluo in mitigating myocardial fibrosis in mice with acute myocardial infarction via neuregulin-1 upregulation and Inhibition of endothelium-interstitial transition.J Mol Histol. 2025 Mar 10;56(2):103. doi: 10.1007/s10735-025-10378-7. J Mol Histol. 2025. PMID: 40063284 Free PMC article.
References
-
- Jones KW, Cain AS, Mitchell JH, Millar RC, Rimmasch HL, French TK, Abbate SL, Roberts CA, Stevenson SR, Marshall D, Lappé DL. Hyperglycemia predicts mortality after CABG: postoperative hyperglycemia predicts dramatic increases in mortality after coronary artery bypass graft surgery. J Diabetes Complicat. 2008;22:365–370. doi: 10.1016/j.jdiacomp.2007.05.006. - DOI - PubMed
LinkOut - more resources
Full Text Sources