

Effect of Lower Limb Alignment in Medial Meniscus-Deficient Knees on Tibiofemoral Contact Pressure
- PMID: 30800688
- PMCID: PMC6378645
- DOI: 10.1177/2325967118824611
Effect of Lower Limb Alignment in Medial Meniscus-Deficient Knees on Tibiofemoral Contact Pressure
Abstract
Background: Degenerative medial meniscal tears and subsequent partial meniscal resection compromise meniscal function and lead to an overload of the medial compartment. In addition, lower limb alignment plays a key role in load distribution between the medial and lateral knee compartments, and varus alignment is a potential risk factor for medial osteoarthritis.
Purpose/hypothesis: The purpose of this biomechanical study was to investigate the effect of valgus and varus alignment on peak pressure and contact area in knees with concomitant horizontal medial meniscal tears and subsequent leaflet resection. It was hypothesized that varus alignment in combination with meniscal loss leads to the highest peak pressure within the medial compartment.
Study design: Controlled laboratory study.
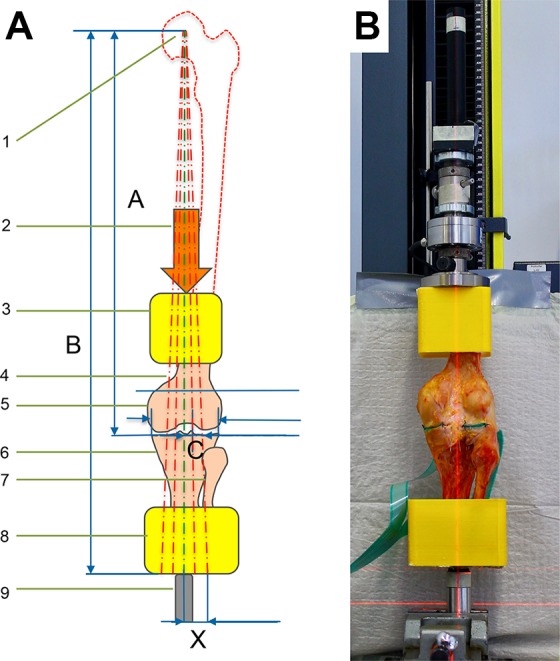
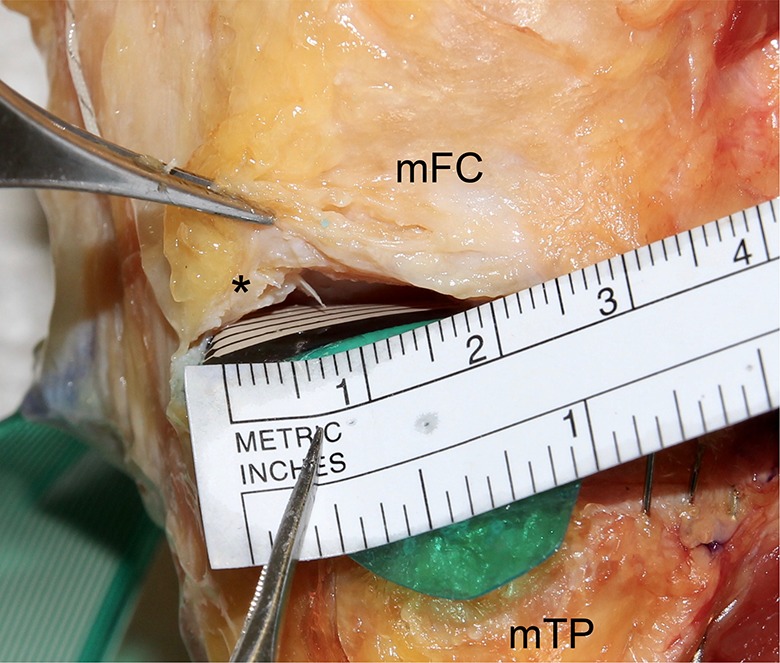
Methods: Six fresh-frozen human cadaveric knees were axially loaded using a 1000-N compressive load in full extension with the mechanical axis rotated to intersect the tibial plateau at 40%, 45%, 50%, 55%, and 60% of its width (TPW) to simulate varus and valgus alignment. Tibiofemoral peak contact pressure and contact area of the medial and lateral compartments were determined using pressure-sensitive foils in each of 4 different meniscal conditions: intact, 15-mm horizontal tear of the posterior horn, inferior leaflet resection, and resection of both leaflets.
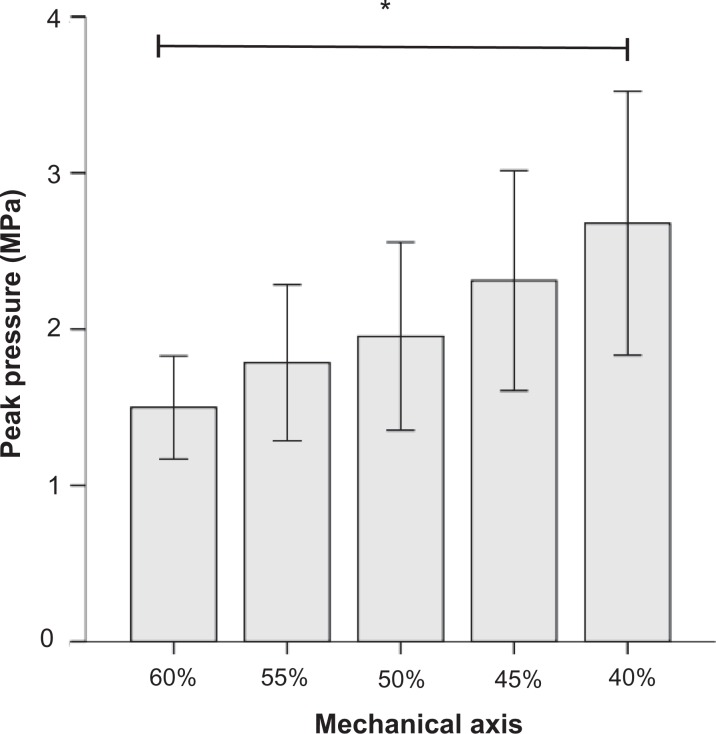
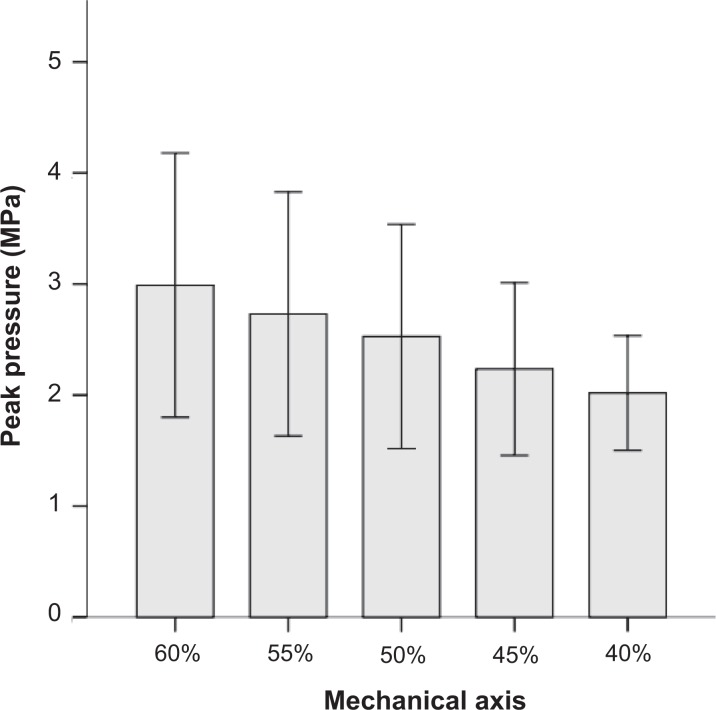
Results: The effect of alignment on peak pressure (normalized to the neutral axis) within the medial compartment in cases of an intact meniscus was measured as follows: varus shift resulted in a mean increase in peak pressure of 18.5% at 45% of the TPW and 37.4% at 40% of the TPW, whereas valgus shift led to a mean decrease in peak pressure of 8.7% at 55% of the TPW and 23.1% at 60% of the TPW. Peak pressure changes between the intact meniscus and resection within the medial compartment was less in valgus-aligned knees (0.21 MPa at 60% TPW, 0.59 MPa at 50% TPW, and 0.76 MPa at 40% TPW). Contact area was significantly reduced after partial meniscal resection in the neutral axis (intact, 553.5 ± 87.6 mm2; resection of both leaflets, 323.3 ± 84.2 mm2; P < .001). This finding was consistent in any alignment.
Conclusion: Both partial medial meniscal resection and varus alignment led to an increase in medial compartment peak pressure. Valgus alignment prevented medial overloading by decreasing contact pressure even after partial meniscal resection. A horizontal meniscal tear did not influence peak pressure and contact area even in varus alignment.
Clinical relevance: As a clinical consequence, partial meniscal resection should be avoided to maintain the original biomechanical behavior, and the mechanical axis should be taken into account if partial meniscectomy is necessary.
Keywords: biomechanical study; contact area; horizontal medial meniscal tear; peak pressure; tibiofemoral joint; valgus; varus.
Conflict of interest statement
One or more of the authors has declared the following potential conflict of interest or source of funding: The Technical University of Munich has received direct funding from the German Arthritis Foundation. This work was supported by the German Research Foundation and the Technical University of Munich within the framework of the Open Access Publishing Program. Funding had no influence on the study design, data collection, or interpretation of the results or the final article. A.B.I. is a consultant for medi GmbH & Co KG and Arthrosurface. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Figures


Similar articles
-
Varus alignment increases medial meniscus extrusion and peak contact pressure: a biomechanical study.Knee Surg Sports Traumatol Arthrosc. 2020 Apr;28(4):1092-1098. doi: 10.1007/s00167-019-05701-1. Epub 2019 Sep 5. Knee Surg Sports Traumatol Arthrosc. 2020. PMID: 31489460
-
Varus alignment aggravates tibiofemoral contact pressure rise after sequential medial meniscus resection.Knee Surg Sports Traumatol Arthrosc. 2020 Apr;28(4):1055-1063. doi: 10.1007/s00167-019-05654-5. Epub 2019 Aug 3. Knee Surg Sports Traumatol Arthrosc. 2020. PMID: 31377827
-
Biomechanical Effects of a Horizontal Medial Meniscal Tear and Subsequent Leaflet Resection.Am J Sports Med. 2016 Apr;44(4):850-4. doi: 10.1177/0363546515623782. Epub 2016 Jan 27. Am J Sports Med. 2016. PMID: 26818450
-
Effects of Lateral Opening-Wedge Distal Femoral Osteotomy on Meniscal Allograft Transplantation: A Biomechanical Evaluation.Orthop J Sports Med. 2023 Jun 5;11(6):23259671231156639. doi: 10.1177/23259671231156639. eCollection 2023 Jun. Orthop J Sports Med. 2023. PMID: 37347021 Free PMC article.
-
The Role of Alignment in Treating Meniscus Pathology.Curr Rev Musculoskelet Med. 2025 Apr;18(4):149-159. doi: 10.1007/s12178-025-09946-x. Epub 2025 Feb 21. Curr Rev Musculoskelet Med. 2025. PMID: 39984811 Free PMC article. Review.
Cited by
-
Internal tibial torsion is associated with medial meniscus posterior horn tears.Knee Surg Sports Traumatol Arthrosc. 2023 Jun;31(6):2251-2256. doi: 10.1007/s00167-022-07173-2. Epub 2022 Sep 25. Knee Surg Sports Traumatol Arthrosc. 2023. PMID: 36153779
-
Free-floating medial meniscus implant kinematics do not change after simulation of medial open-wedge high tibial osteotomy and notchplasty.J Exp Orthop. 2023 Feb 9;10(1):13. doi: 10.1186/s40634-023-00576-1. J Exp Orthop. 2023. PMID: 36757624 Free PMC article.
-
A narrative review of lateral meniscus root tears and extrusion: techniques and outcomes.Ann Jt. 2022 Apr 15;7:15. doi: 10.21037/aoj-20-112. eCollection 2022. Ann Jt. 2022. PMID: 38529138 Free PMC article. Review.
-
Varus alignment increases medial meniscus extrusion and peak contact pressure: a biomechanical study.Knee Surg Sports Traumatol Arthrosc. 2020 Apr;28(4):1092-1098. doi: 10.1007/s00167-019-05701-1. Epub 2019 Sep 5. Knee Surg Sports Traumatol Arthrosc. 2020. PMID: 31489460
-
Influence of Menisci on Tibiofemoral Contact Mechanics in Human Knees: A Systematic Review.Front Bioeng Biotechnol. 2021 Dec 3;9:765596. doi: 10.3389/fbioe.2021.765596. eCollection 2021. Front Bioeng Biotechnol. 2021. PMID: 34926419 Free PMC article. Review.
References
-
- Agneskirchner JD, Hurschler C, Wrann CD, Lobenhoffer P. The effects of valgus medial opening wedge high tibial osteotomy on articular cartilage pressure of the knee: a biomechanical study. Arthroscopy. 2007;23(8):852–861. - PubMed
-
- Allaire R, Muriuki M, Gilbertson L, Harner CD. Biomechanical consequences of a tear of the posterior root of the medial meniscus: similar to total meniscectomy. J Bone Joint Surg Am. 2008;90(9):1922–1931. - PubMed
-
- Arno S, Bell CP, Uquillas C, Borukhov I, Walker PS. Tibiofemoral contact mechanics following a horizontal cleavage lesion in the posterior horn of the medial meniscus. J Orthop Res. 2015;33(4):584–590. - PubMed
-
- Beamer BS, Walley KC, Okajima S, et al. Changes in contact area in meniscus horizontal cleavage tears subjected to repair and resection. Arthroscopy. 2017;33(3):617–624. - PubMed
-
- Bedi A, Kelly NH, Baad M, et al. Dynamic contact mechanics of the medial meniscus as a function of radial tear, repair, and partial meniscectomy. J Bone Joint Surg Am. 2010;92(6):1398–1408. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
