

Online Digital Education for Postregistration Training of Medical Doctors: Systematic Review by the Digital Health Education Collaboration
- PMID: 30801252
- PMCID: PMC6410118
- DOI: 10.2196/13269
Online Digital Education for Postregistration Training of Medical Doctors: Systematic Review by the Digital Health Education Collaboration
Abstract
Background: Globally, online and local area network-based (LAN) digital education (ODE) has grown in popularity. Blended learning is used by ODE along with traditional learning. Studies have shown the increasing potential of these technologies in training medical doctors; however, the evidence for its effectiveness and cost-effectiveness is unclear.
Objective: This systematic review evaluated the effectiveness of online and LAN-based ODE in improving practicing medical doctors' knowledge, skills, attitude, satisfaction (primary outcomes), practice or behavior change, patient outcomes, and cost-effectiveness (secondary outcomes).
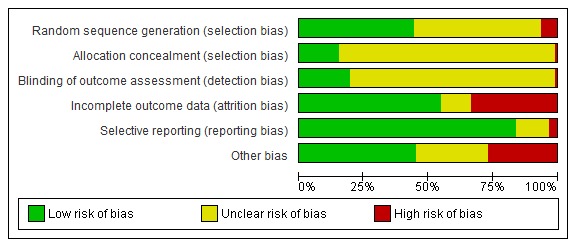
Methods: We searched seven electronic databased for randomized controlled trials, cluster-randomized trials, and quasi-randomized trials from January 1990 to March 2017. Two review authors independently extracted data and assessed the risk of bias. We have presented the findings narratively. We mainly compared ODE with self-directed/face-to-face learning and blended learning with self-directed/face-to-face learning.
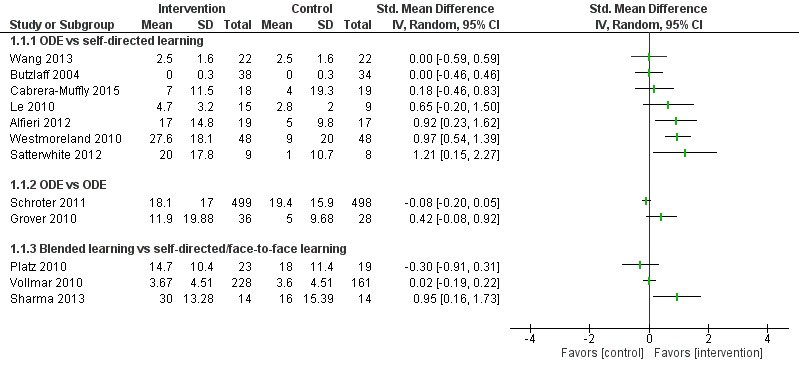
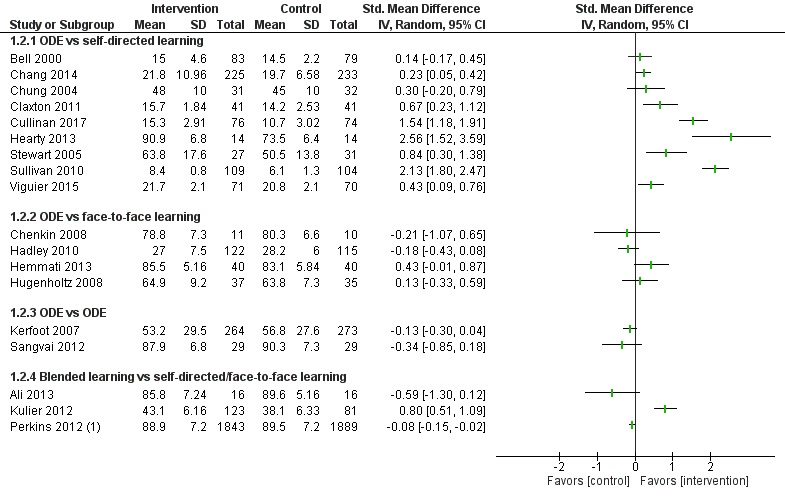
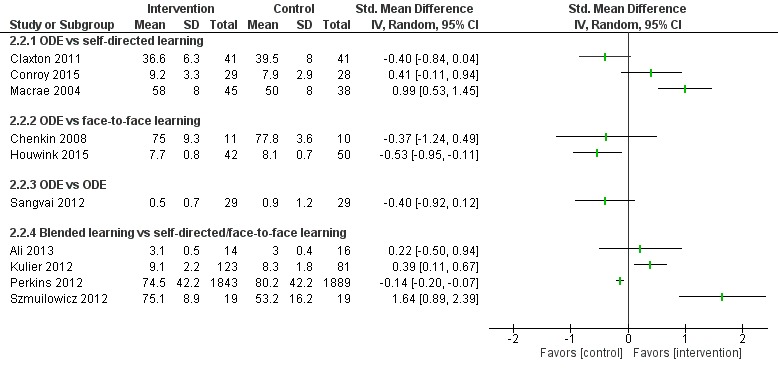
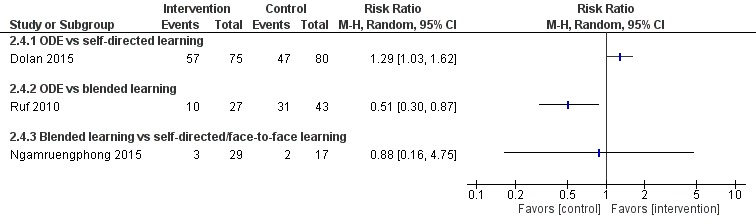
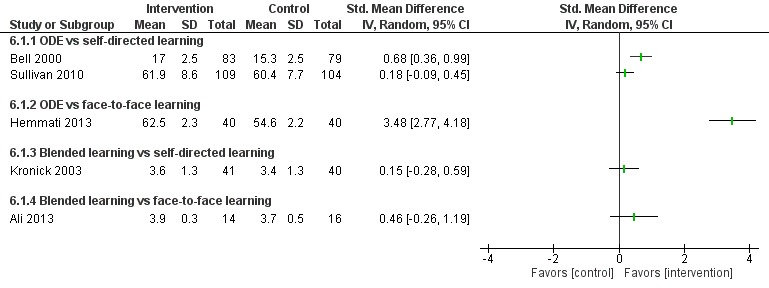
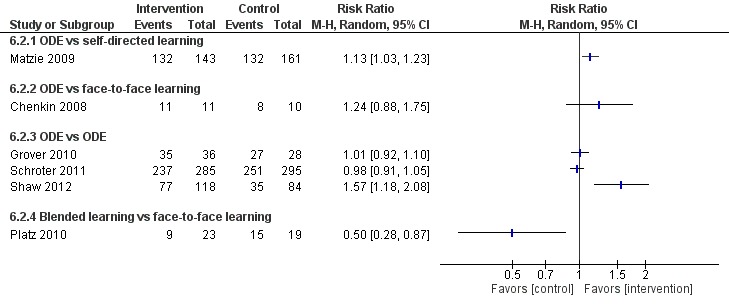
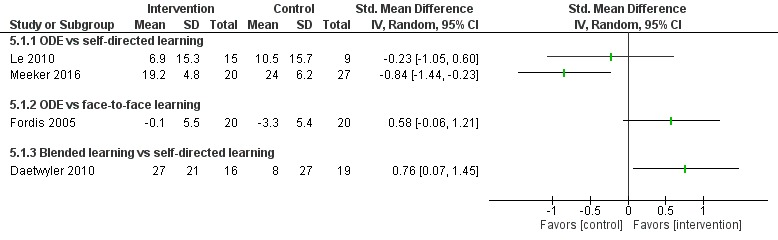
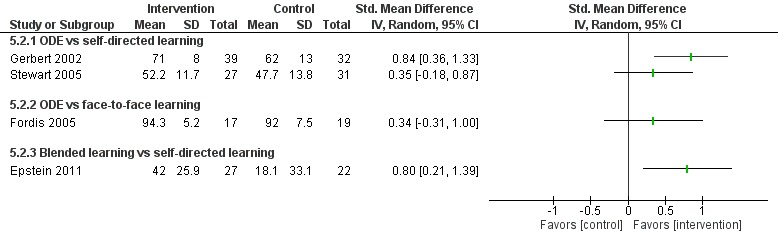
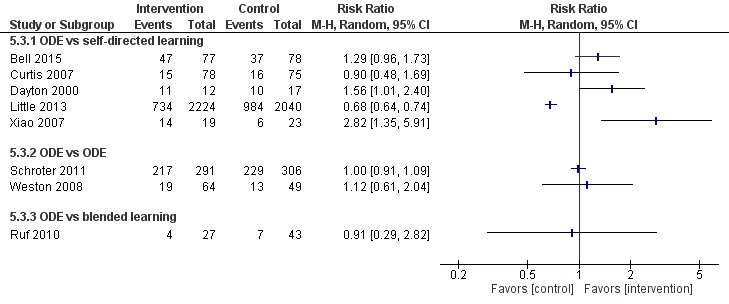
Results: A total of 93 studies (N=16,895) were included, of which 76 compared ODE (including blended) and self-directed/face-to-face learning. Overall, the effect of ODE (including blended) on postintervention knowledge, skills, attitude, satisfaction, practice or behavior change, and patient outcomes was inconsistent and ranged mostly from no difference between the groups to higher postintervention score in the intervention group (small to large effect size, very low to low quality evidence). Twenty-one studies reported higher knowledge scores (small to large effect size and very low quality) for the intervention, while 20 studies reported no difference in knowledge between the groups. Seven studies reported higher skill score in the intervention (large effect size and low quality), while 13 studies reported no difference in the skill scores between the groups. One study reported a higher attitude score for the intervention (very low quality), while four studies reported no difference in the attitude score between the groups. Four studies reported higher postintervention physician satisfaction with the intervention (large effect size and low quality), while six studies reported no difference in satisfaction between the groups. Eight studies reported higher postintervention practice or behavior change for the ODE group (small to moderate effect size and low quality), while five studies reported no difference in practice or behavior change between the groups. One study reported higher improvement in patient outcome, while three others reported no difference in patient outcome between the groups. None of the included studies reported any unintended/adverse effects or cost-effectiveness of the interventions.
Conclusions: Empiric evidence showed that ODE and blended learning may be equivalent to self-directed/face-to-face learning for training practicing physicians. Few other studies demonstrated that ODE and blended learning may significantly improve learning outcomes compared to self-directed/face-to-face learning. The quality of the evidence in these studies was found to be very low for knowledge. Further high-quality randomized controlled trials are required to confirm these findings.
Keywords: effectiveness; internet; medical education; randomized controlled trials; systematic review.
©Pradeep Paul George, Olena Zhabenko, Bhone Myint Kyaw, Panagiotis Antoniou, Pawel Posadzki, Nakul Saxena, Monika Semwal, Lorainne Tudor Car, Nabil Zary, Craig Lockwood, Josip Car. Originally published in the Journal of Medical Internet Research (http://www.jmir.org), 25.02.2019.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures




References
-
- Bleakley A, Bligh J, Browne J. Medical Education For The Future. Berlin, Germany: Springer Science & Business Media; 2019.
-
- Chen N, Wang Y. Cyber schooling framework: Improving mobility and situated learning. Intl Journal of Eng Ed. 2007;23:421–33. doi: 10.1109/ICALT.2005.99. https://www.computer.org/csdl/proceedings/icalt/2005/2338/00/23380290-ab... - DOI
-
- Clark D. Psychological myths in e-learning. Med Teach. 2002 Nov;24(6):598–604. doi: 10.1080/0142159021000063916. https://www.tandfonline.com/doi/abs/10.1080/0142159021000063916 K8TBJ3RQW2HMQD9T - DOI - DOI - PubMed
-
- Cook DA. The research we still are not doing: an agenda for the study of computer-based learning. Acad Med. 2005 Jun;80(6):541–8.80/6/541 - PubMed
-
- Sangrà A, Vlachopoulos D, Cabrera N. Building an inclusive definition of e-learning: an approach to the conceptual framework. Int Rev Res Open Distance Learn. 2012;13:a.
