

Analysis of Drivers of Disenrollment and Plan Switching Among Medicare Advantage Beneficiaries
- PMID: 30801625
- PMCID: PMC6450306
- DOI: 10.1001/jamainternmed.2018.7639
Analysis of Drivers of Disenrollment and Plan Switching Among Medicare Advantage Beneficiaries
Abstract
Importance: How often enrollees with complex care needs leave the Medicare Advantage (MA) program and what might drive their decisions remain unknown.
Objective: To characterize trends in switching to and from MA among high-need beneficiaries and to evaluate the drivers of disenrollment decisions.
Design, setting, and participants: This cross-sectional study of MA and traditional Medicare (TM) enrollees from January 1, 2014, through December 31, 2015, used a multinomial logit regression stratified by Medicare-Medicaid eligibility status. All 14 589 645 non-high-need MA enrollees and 1 302 470 high-need enrollees in the United States who survived until the end of 2014 were eligible for the analysis. Data were analyzed from November 1, 2017, through August 1, 2018.
Exposures: Enrollee dual eligibility and high-need status (based on complex chronic conditions, multiple morbidities, use of health care services, functional impairment, and frailty indicators), MA plan star rating, and cost sharing.
Main outcomes and measures: The proportion of enrollees who disenrolled into TM, remained in the same MA plan, or who switched plans within the MA program.
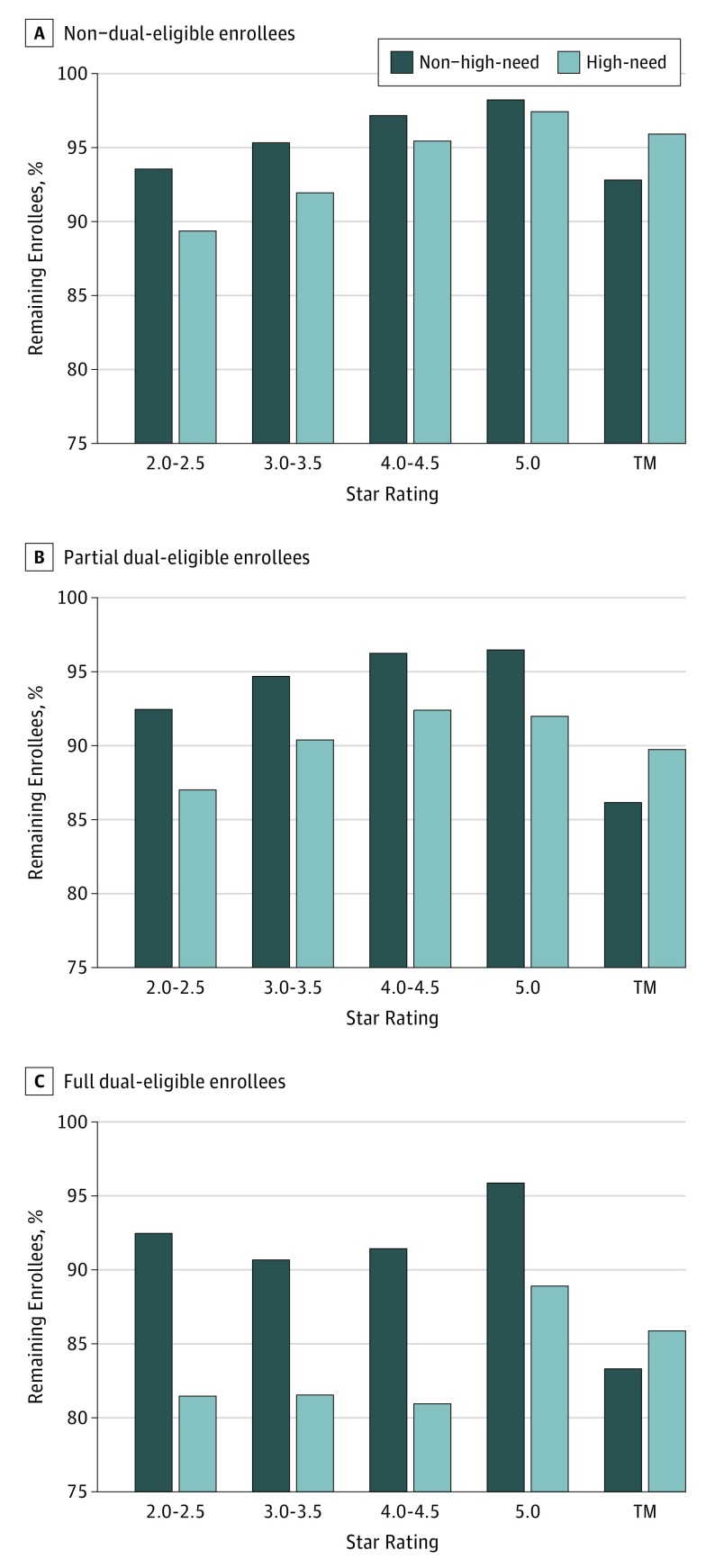
Results: A total of 13 901 816 enrollees were included in the analysis (56.2% women; mean [SD] age, 70.9 [9.9] years). Among the 1 302 470 high-need enrollees, an adjusted 4.6% (95% CI, 4.5%-4.6%) of Medicare-only and 14.8% (95% CI, 14.5%-15.0%) of Medicare-Medicaid members switched from MA to TM compared with 3.3% (95% CI, 3.3%-3.3%) and 4.6% (95% CI, 4.5%-4.7%), respectively, among non-high-need enrollees. Among enrollees in low-quality plans, 23.0% (95% CI, 22.3%-23.9%) of Medicare and 42.8% (95% CI, 40.5%-45.1%) of dual-eligible high-need enrollees left MA. Even in high-quality plans, high-need members disenrolled at higher rates than non-high-need members (4.9% [95% CI, 4.6%-5.2%] vs 1.8% [95% CI, 1.8%-1.9%] for Medicare-only enrollees and 11.3% vs 2.4% dual eligible enrollees). Enrollment in a 5.0-star rated plan was associated with a 30.1-percentage point reduction (95% CI, -31.7 to -28.4 percentage points) in the probability of disenrollment among high-need individuals. A $100 increase in monthly premiums was associated with a 33.9-percentage point increase (95% CI, -34.9 to -33.0 percentage points) in the likelihood of switching plans, and a small reduction in the likelihood of disenrolling (-2.7 percentage points; 95% CI, -3.2 to -2.2 percentage points). Among Medicare-Medicaid eligible participants, 14.1% (95% CI, 14.0%-14.2%) of high-need and 16.7% (95% CI, 16.6%-16.7%) of non-high-need enrollees switched from TM to MA.
Conclusions and relevance: Results of this study suggest that substantially higher disenrollment from MA plans occurs among high-need and Medicare-Medicaid eligible enrollees. This study's findings suggest that star ratings have the strongest association with disenrollment trends, whereas increases in monthly premiums are associated with greater likelihood of switching plans.
Conflict of interest statement
Figures
References
-
- Anderson GF, Ballreich J, Bleich S, et al. Attributes common to programs that successfully treat high-need, high-cost individuals. Am J Manag Care. 2015;21(11):e597-e600. - PubMed
