

Invasive Fungal Infection After Lung Transplantation: Epidemiology in the Setting of Antifungal Prophylaxis
- PMID: 30801642
- PMCID: PMC6912154
- DOI: 10.1093/cid/ciz156
Invasive Fungal Infection After Lung Transplantation: Epidemiology in the Setting of Antifungal Prophylaxis
Abstract
Background: Lung transplant recipients commonly develop invasive fungal infections (IFIs), but the most effective strategies to prevent IFIs following lung transplantation are not known.
Methods: We prospectively collected clinical data on all patients who underwent lung transplantation at a tertiary care academic hospital from January 2007-October 2014. Standard antifungal prophylaxis consisted of aerosolized amphotericin B lipid complex during the transplant hospitalization. For the first 180 days after transplant, we analyzed prevalence rates and timing of IFIs, risk factors for IFIs, and data from IFIs that broke through prophylaxis.
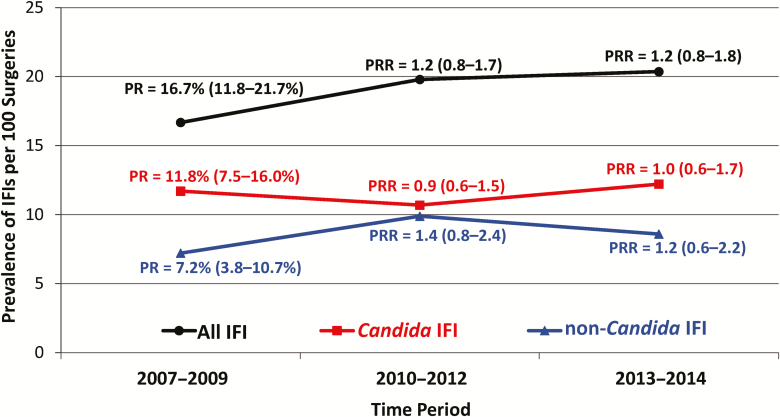
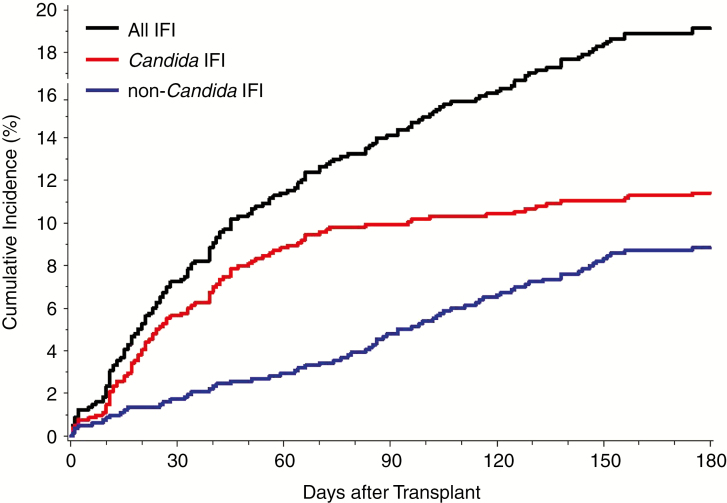
Results: In total, 156 of 815 lung transplant recipients developed IFIs (prevalence rate, 19.1 IFIs per 100 surgeries, 95% confidence interval [CI] 16.4-21.8%). The prevalence rate of invasive candidiasis (IC) was 11.4% (95% CI 9.2-13.6%), and the rate of non-Candida IFIs was 8.8% (95% CI 6.9-10.8%). First episodes of IC occurred a median of 31 days (interquartile range [IQR] 16-56 days) after transplant, while non-Candida IFIs occurred later, at a median of 86 days (IQR 40-121 days) after transplant. Of 169 IFI episodes, 121 (72%) occurred in the absence of recent antifungal prophylaxis; however, IC and non-Candida breakthrough IFIs were observed, most often representing failures of micafungin (n = 16) and aerosolized amphotericin B (n = 24) prophylaxis, respectively.
Conclusions: Lung transplant recipients at our hospital had high rates of IFIs, despite receiving prophylaxis with aerosolized amphotericin B lipid complex during the transplant hospitalization. These data suggest benefit in providing systemic antifungal prophylaxis targeting Candida for up to 90 days after transplant and extending mold-active prophylaxis for up to 180 days after surgery.
Keywords: invasive fungal infection; lung transplantation; prophylaxis.
© The Author(s) 2019. Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions, e-mail: journals.permissions@oup.com.
Figures
Comment in
-
Invasive Fungal Infections in Lung Transplant Recipients.Clin Infect Dis. 2021 Jan 27;72(2):365-366. doi: 10.1093/cid/ciaa603. Clin Infect Dis. 2021. PMID: 33501955 No abstract available.
-
Reply to Marinelli and Rotstein.Clin Infect Dis. 2021 Jan 27;72(2):366-367. doi: 10.1093/cid/ciaa605. Clin Infect Dis. 2021. PMID: 33501960 No abstract available.
References
-
- Yusen RD, Edwards LB, Kucheryavaya AY, et al. The registry of the international society for heart and lung transplantation: thirty-second official adult lung and heart-lung transplantation report–2015; focus theme: early graft failure. J Heart Lung Transplant 2015; 34:1264–77. - PubMed
-
- Yeung JC, Cypel M, Waddell TK, van Raemdonck D, Keshavjee S. Update on donor assessment, resuscitation, and acceptance criteria, including novel techniques–non-heart-beating donor lung retrieval and ex vivo donor lung perfusion. Thorac Surg Clin 2009; 19:261–74. - PubMed
-
- Fuehner T, Kuehn C, Welte T, Gottlieb J. ICU care before and after lung transplantation. Chest 2016; 150:442–50. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
